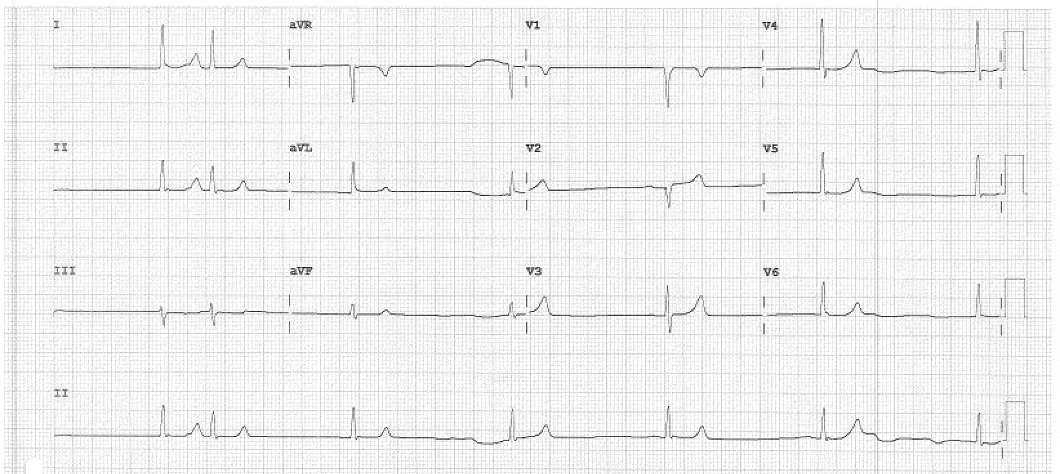
Case Presentation: A 60-year-old male with chronic kidney disease 3a, hypertension (HTN) and type 2 diabetes was found unresponsive at work. The patient’s home medications were carvedilol, nifedipine, spironolactone and valsartan for his resistant HTN. Initial evaluation revealed undifferentiated shock with an inappropriately low heart rate of 40 beats per minute. Labs showed potassium of 8.1 with creatinine of 2.7 and normal glucose. Electrocardiogram revealed complete heart block with junctional escape rhythm without other features of hyperkalemia (Image 1). Transthoracic echocardiogram revealed left ventricular hypertrophy with abnormal relaxation and an ejection fraction of 50-55%, but no other cardiac defects. The patient was given atropine without improvement. Transcutaneous pacing was ineffective, and he was started on epinephrine and dopamine for inotropic and chronotropic support. Medical management failed to treat hyperkalemia and he subsequently underwent urgent dialysis. Bradycardia resolved with resolution of hyperkalemia.
Discussion: BRASH (bradycardia, renal failure, use of an atrioventricular (AV) nodal blocker, shock, and hyperkalemia) is an uncommon clinical syndrome presenting with bradycardia and shock. It is a distinct entity from pure hyperkalemia or AV nodal blockade toxicity. BRASH is usually precipitated by acute kidney injury (AKI) in the setting of chronic kidney disease, often precipitated by only mild volume depletion. The AKI leads to a positive feedback loop with downward effects including hyperkalemia, and in the setting of AV nodal blockers, results in progressive bradycardia and eventually hypotension and shock. The defining feature of BRASH is AV nodal blocking agents, such as carvedilol in our case, along with hyperkalemia due to AKI. Management of our patient’s underlying hyperkalemia by emergent dialysis corrected his bradycardia and resultant shock.
Conclusions: Prompt recognition of BRASH can lead to avoidance of a cyclical phenomenon leading to a life-threatening situation. We present a classic case of BRASH often requiring hemodialysis and vasopressor support. The mainstay treatment for BRASH is treating the hyperkalemia promptly.