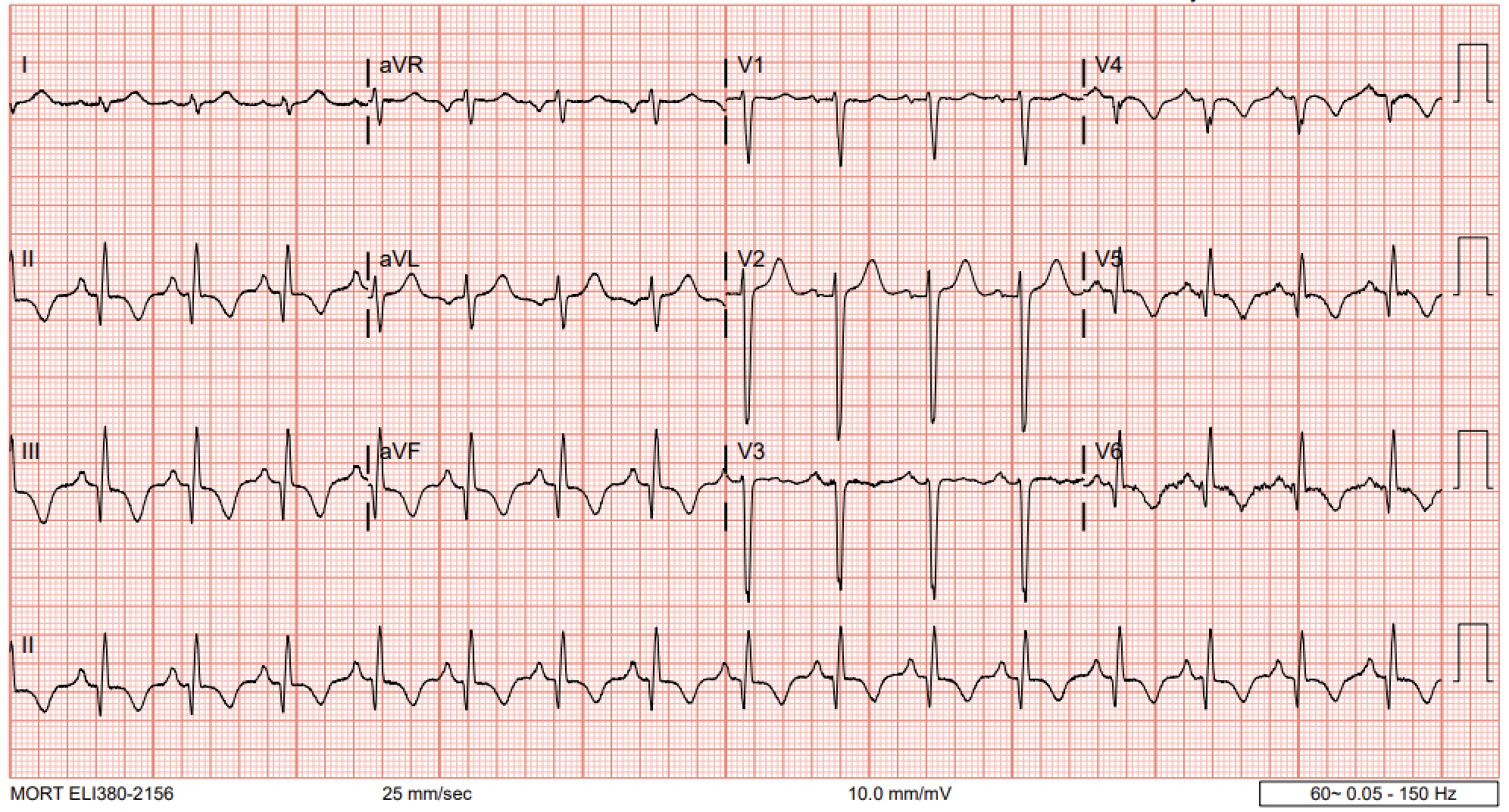
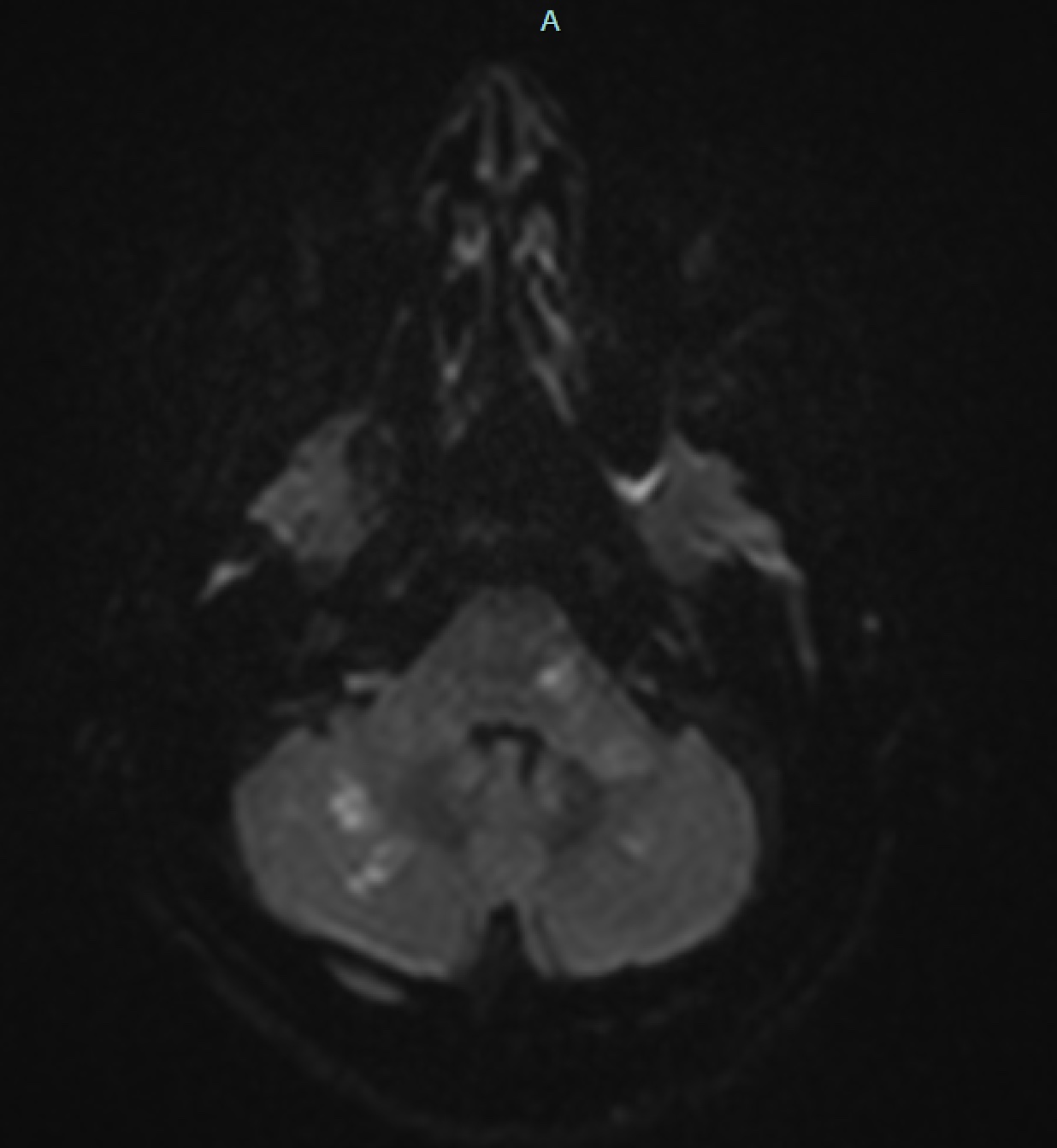
Case Presentation: A 72-year-old man with hypertension and tobacco use presented to the emergency room with three days of nausea, vomiting, substernal chest pain, and thoracic back pain, following weeks of worsening vertigo. He also described a year of progressive tinnitus, diplopia, unsteady gait, and restless legs. Vital signs were stable. Physical exam revealed bilateral horizontal nystagmus, a positive Romberg sign, and ataxic gait.Initial labs showed white blood cell count of 25 × 10⁹/L, hemoglobin 23 g/dL, platelets 841 × 10⁹/L, total bilirubin 3.7 mg/dL, and elevated brain natriuretic peptide at 743 pg/mL. Troponin rose from 0.08 ng/mL to 0.24 ng/mL. The electrocardiogram showed diffuse T wave inversions without ST changes and loss of R waves in V2-V3. Transthoracic echocardiogram revealed a 45% ejection fraction with akinesis of the apical septal and lateral walls,and hypokinesis of the basal inferior wall. Computed tomography of the head showed chronic lacunar and cerebellar infarcts while computed tomography of the chest showed moderate coronary artery atherosclerosis. Cardiac catheterization demonstrated severe left anterior descending and right coronary artery disease. Further workup revealed an iron level of 25 μg/dL, ferritin 14 ng/mL, uric acid 8 mg/dL, lactate dehydrogenase 294 U/L, and a low erythropoietin level of 2.1 mIU/mL. JAK2 mutation testing confirmed polycythemia vera (PV). This patient’s acute chest pain in the context of progressive vasomotor symptoms, cardiac workup, and abnormal lab findings led to a diagnosis of non-ST elevation myocardial infarction (NSTEMI) secondary to PV. He was treated with hydroxyurea, serial phlebotomies, and medical management of his coronary artery disease.
Discussion: Polycythemia vera is a chronic myeloproliferative neoplasm caused by a gain-of-function mutation in the JAK2 gene. This mutation drives erythropoietin-independent proliferation of red blood cells, platelets, and granulocytes, leading to increased blood viscosity, endothelial damage, and hypercoagulability. These changes predispose patients to major adverse cardiovascular events, including myocardial infarction, stroke, and heart failure.Thrombotic complications in PV arise from components of Virchow’s triad: venous stasis, endothelial injury, and hypercoagulability. Microvascular dysfunction further contributes to ischemic events through impaired coronary flow reserve, abnormal vasodilation, and enhanced vasoconstrictor responsiveness. Up to 27.6% of patients hospitalized with PV have coexisting heart failure, which is associated with higher length of stay and mortality. Myocardial infarction has been reported in 11.4% of PV patients, often in conjunction with traditional atherosclerotic risk factors like hypertension and tobacco use, as seen in this case.However, myocardial infarction in PV can also occur in patients without coronary artery disease due to coronary microvascular dysfunction. The patient discussed here had significant atherosclerosis compounded by PV-related hyperviscosity, amplifying his risk of major adverse cardiovascular events.
Conclusions: This case highlights the importance of recognizing polycythemia vera in patients presenting with myocardial infarction or stroke, particularly when accompanied by symptoms of microvascular dysfunction such as vertigo or burning extremity pain. Early identification and management of PV are critical to reducing cardiovascular complications and improving long-term outcomes.