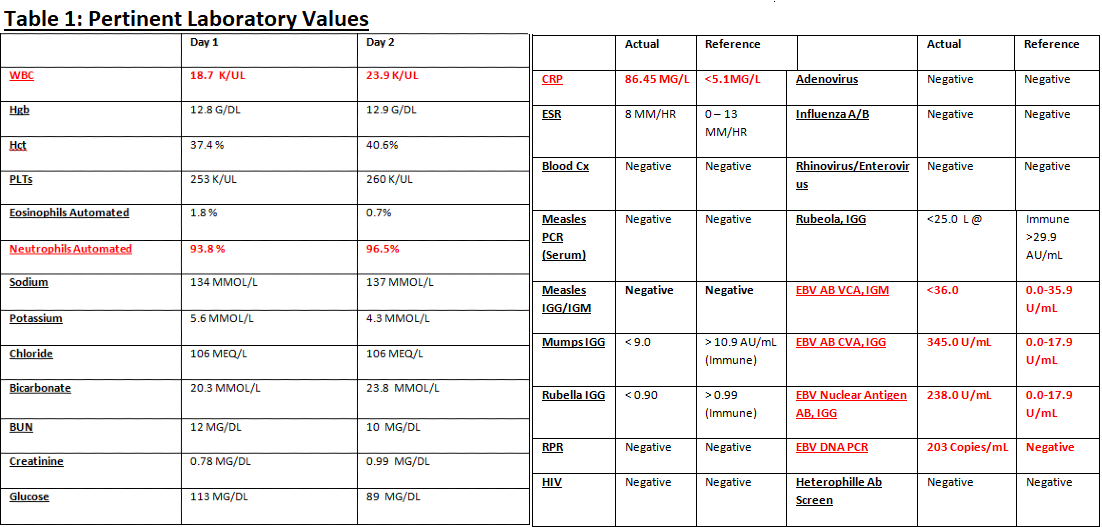
Case Presentation: The patient is a 30 year American Born, Middle Eastern male with PMH Acute Generalized Exanthematous Pustulsosis (AGEP) that comes into hospital with high fevers and diffuse pruritic rash. In January of 2019, the patient, while being treated for pharyngitis, developed a pruritic, pustular rash, after treatment with amoxicillin/clavulanic acid. He was diagnosed with AGEP, the medication was discontinued and his sore throat and rash resolved. In late March 2019, the patient was admitted for presumed streptococcal pharyngitis infection and was treated alternatively with IV clindamycin, in-hospital, and he was discharged on oral Clindamycin. He presented again in early April with facial swelling and redness that developed on his face, arms, trunk and legs. The patient noted only the aforementioned allergy to penicillin. He took no medications nor did he use any drugs or alcohol. He was a former smoker (quit the previous year). He was heterosexual and had no recent travel. In the emergency department, his vitals were noted as such: Tmax was 101.6 F. Exam on admission was noted for diffuse erythematous maculopapular morbilliform rash. Labs were remarkable for a WBC of 18.7. It was suspected that this was a repeat presentation of his AGEP. With 12 hours, the quality of the patient’s rash changed to pustules on the patient’s face arms, and trunk. Patient’s fever came up to 103.2 and his WBC increased to 23.9. Measles PCR was negative as was Rapid Strep Test and Throat Culture. Patient had no antibody titers to Measles, Mumps or Rubella. This was thought to be a new presentation of AGEP due to clindamycin. He was started on oral steroids. By the 4th day of admission, the rash came to resolve. He was discharged with a 7 day course of topical and oral steroids. It was found later that the patient not only had positive EBV VCA IGG Antibodies and Nuclear Antigen Antibodies, He was noted to have Viral DNA PCR positive for EBV DNA. EBV IgM VCA was negative.
Discussion: AGEP is rare condition entailing diffuse pustular rash on that can encompass the face, extremities, and trunk often associated with edematous erythema, high fevers, and elevated neutrophils. This is due to apoptosis of the keratinocytes in the epidermis, recruitment of Neutrophils to the skin surface and pustule formation. Risk factors include, exposure pristinamycin, penicillins, quinolones, and others drugs. Most other cases of AGEP are viral in nature or idiopathic. Recurrent AGEP is only rarely documented in the medical literature. In the patient, positive EBV VCA IgG and Nuclear antigen Antibodies with negative VCA IgM seem to indicate that primary diagnosis on his first admission in March was Epstein-Bar Virus infection. The presence EBV DNA (detected through PCR) can be elevated in the presence of infectious mononucleosis early in the disease course pointing to a likely reactivation event. It is possible that our case patient is the victim of a “second hit”; with virally mediated dysregulation of T-cell Activity followed by exposure to a novel antibiotic.
Conclusions: In this case, we have patient that has rare presentation to the hospital with a recurrent AGEP in patient with exposure to clindamycin and EBV. Diagnostic uncertainty as made it difficult to label the exact insult leading to disease presentation. It is possible that the patient was the victim of combination of factors leading to dysregulated T-cell activity within the epidermis. Further research is need into precise mechanism of drug induced/virally mediated cytotoxic response on the skin.