Background: Hospital Medicine is being increasingly involved in improving various metrices of inpatient care such as length of stay and cost of care. Patients who do not meet ‘inpatient criteria’ often contribute to significant financial costs to hospitals and remain in ‘observation status’ during their hospital stay. Observations units which were introduced by emergency doctors as chest pain units as a part of Emergency Departments, are now being expanded to include other diagnoses and are being staffed by hospitalists. Not much is known about financial impact of observation units though they have been shown to improve length of stay in some of the previously published work. We report results of an observation unit at a 900-bed tertiary care hospital staffed by hospitalists and nurse practitioners.
Methods: Observations status patients with variety of diagnoses except placement needs were admitted on a dedicated observation unit. Diagnoses such as chest pain, NSTEMI, TIA, simple pneumonia, asthma exacerbation, A fib with rapid rate, COPD etc to mention a few were included on the unit. Unit had 24 beds during the year 2018 and 40 beds during 2019. 40 bed unit was staffed with 2 MDs and 3 Nurse practitioners. We created a leadership pathway for successful triaging of patients from emergency room to observation unit and provided necessary testing availability to these patients in a timely manner.
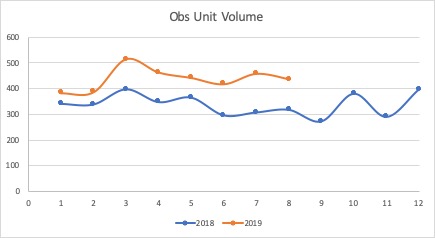
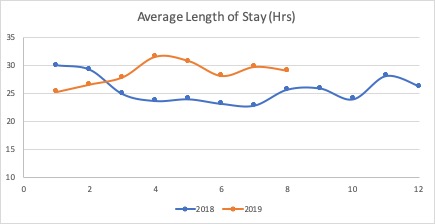
Results: During the year 2018, 3375 patients were cared on a 24 bed Observation unit with an average length of stay of 25.6 hours. During the year 2019, unit was expanded to 40 beds and we saw 3119 patients through August 2019 with average length of stay of 28.4 hours. Length of stay for patients in observation status but not on observation unit was 42.7 hours for 2018 and 44.8 hours for year to date in 2019 respectively. Based on results of the observation unit during the year 2015, we were able to show an annual cost saving of about 2 million dollars by caring for patients on dedicated observation unit (financial calculations not provided here).
Conclusions: We thus demonstrate for the first-time, significant reductions in the cost of care and length of stay by implementation of a dedicated observation unit at 900 bed tertiary care hospital.