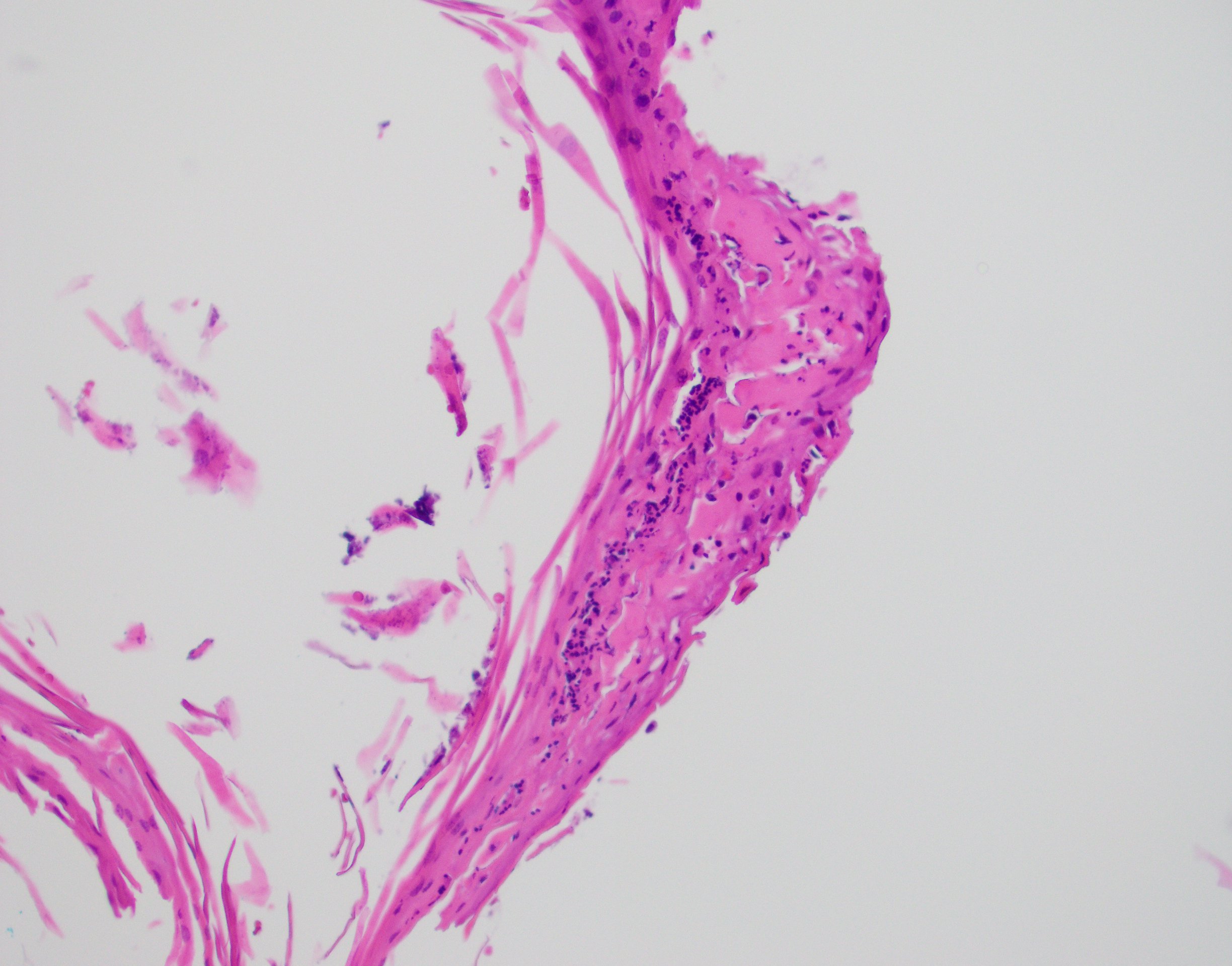
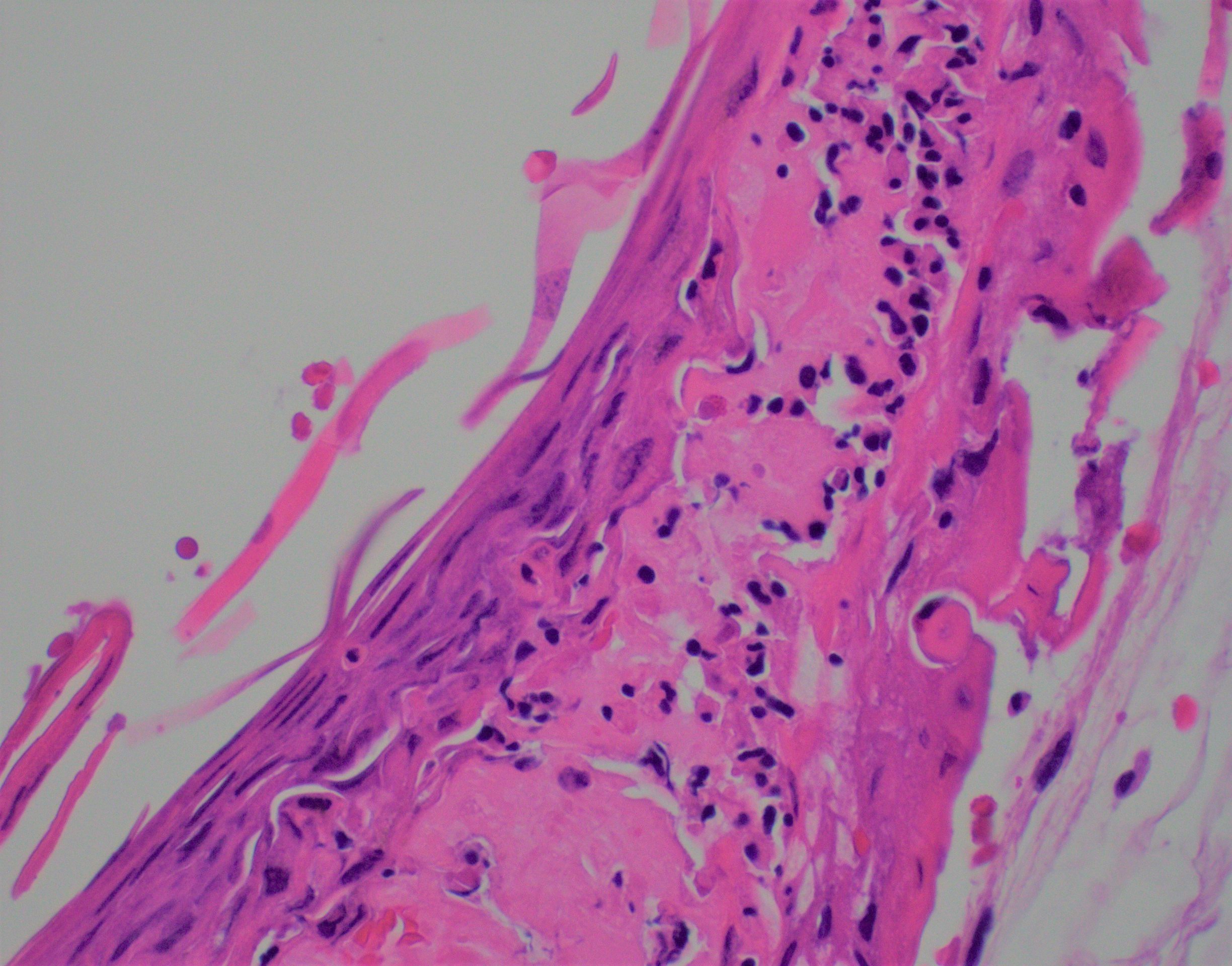
Case Presentation: A 90-year female with a recent onset of vancomycin induced hypersensitivity reaction presents to the ED with sepsis and generalized disseminated rash. She recently underwent a surgery that was complicated with pseudomonas infection and was treated with vancomycin and Zosyn. However, she developed a pruritic, erythematous macular rash on her abdomen and vancomycin was discontinued. The current presentation was preceded with angioedema, swelling of the face and lips that was relieved after symptomatic treatment, however a week later the patient was readmitted to ER for symptom recurrence. Physical examination revealed pruritic, erythematous, macular rash involving over 50% of her body surface area with targeted lesions on her palms. Her initial blood work was significant for leukocytosis, thrombocytopenia, and an elevated creatinine concerning for acute kidney injury. In our patient, RegiSCAR score was “probable” that was calculated on eosinophilia > 1500/uL (2 points), rash involving > 50% of body surface (1 point), facial edema and desquamation (1 point), multiorgan involvement (2 points), skin biopsy showing alternative diagnosis (negative one point). Skin biopsy showed superficial fragments of squamous epithelium with necrotic keratinocytes and a mixed inflammatory infiltrate comprised of neutrophils, lymphocytes and occasional eosinophils. The reported pathologic findings were most suggestive of EM. Treatment with oral and topical steroids resulted in symptom resolution and her cell counts normalized with resolution of her rash.
Discussion: Erythema multiforme (EM) is an immune-mediated disorder most often induced by infection and rarely with medications. The syndrome of Drug reaction with eosinophilia and systemic symptoms (DRESS) is a rare, potentially fatal hypersensitivity reaction that typically manifests after a long latency period from drug exposure, with an estimated incidence of 1 in 1,000 to 1 in 10,000 drug exposures[1, 2]. It is an immune-mediated reaction characterized by morbilliform rash, eosinophilia, fever, and lymphadenopathy that can result in multi-organ failure[3]. Scoring systems such as RegiSCAR have been validated to classify DRESS as possible, probable, or definite[4]. We report a unique case of DRESS syndrome with overlapping EM findings. The interesting features of this case include Vancomycin induced DRESS[5], “probable” RegiSCAR score and skin biopsy positive for EM. Our case raises the question of the usefulness of RegiSCAR with “probable” score in the diagnosis of DRESS with overlapping EM features.
Conclusions: In conclusion, we present a unique case of EM with DRESS-like features. This is a rare presentation of two unique severe cutaneous reactions to the same medication that presented concurrently. This case emphasizes the importance of precise diagnosis of any and all severe skin reactions to an offending medication, as each reaction carries a different degree of mortality risk.