Background: The Hospital Discharge Day Management Service (CPT code 99238 or 99239) is a face-to-face evaluation and management (E/M) service provided to the patient by his/her attending physician on the day of discharge. The two codes differ based on the amount of documented time physicians spend in coordinating care and discharge services of either 30 minutes or less (CPT 99238) or greater than 30 minutes (CPT 99239). In 2015, the national average for the use of 99239 is 56%, with a charge of $385, compared to $280 for 99238. The aim of this study was to explore associations between the time spent in coordinating care at the patient’s discharge and the patient’s age, race, gender, insurance, disposition, length of stay, and time patient left the hospital.
Methods: A retrospective chart review evaluated patients admitted to a suburban non-teaching hospital in a major Midwestern health system who were discharged by a hospitalist between June 1, 2014 and June 30, 2015 with a billing code of 99238 or 99239. Demographic information was collected on all patients. Race included white, black, other, and declined/unknown. The insurance payer category included Medicare, Blue Cross, a health care system HMO, and other. The disposition category included home or self-care, home health care, skilled nursing facility, or other. Mean length of stay, average time of discharge, and proportion of patients discharged prior to noon were evaluated. A Chi-squared analysis was used to evaluate for significant associations between billing code and clinical and demographic variables.
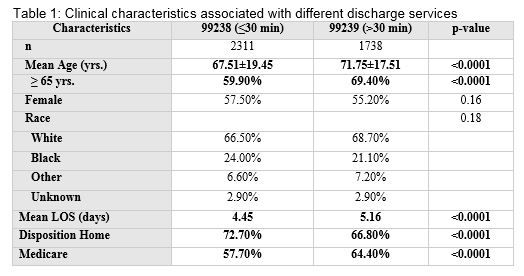
Results: A total of 4976 patients were discharged, with 4049 (81%) having hospitalists as the discharge attending. Among the patients discharged by hospitalists, 1738 (43%) carried the 99239 code. There were significant statistical differences (p<0.0001) seen in age, mean length of stay, disposition, and payer (see Table 1). There was no statistical difference in average time of discharge (99238: 3:29pm vs 99239: 3:34pm; p=0.53) or proportion of patients discharged prior to noon (99238: 12.3% vs. 99239: 11.4%; p=0.43).
Conclusions: Based on our retrospective analysis, there were significant associations between a longer documented time of discharge in patients of greater age, longer length of stay, or patients not going home. Future research should evaluate whether patients with longer documented discharge services have different risk adjusted outcomes following transition from the hospital.