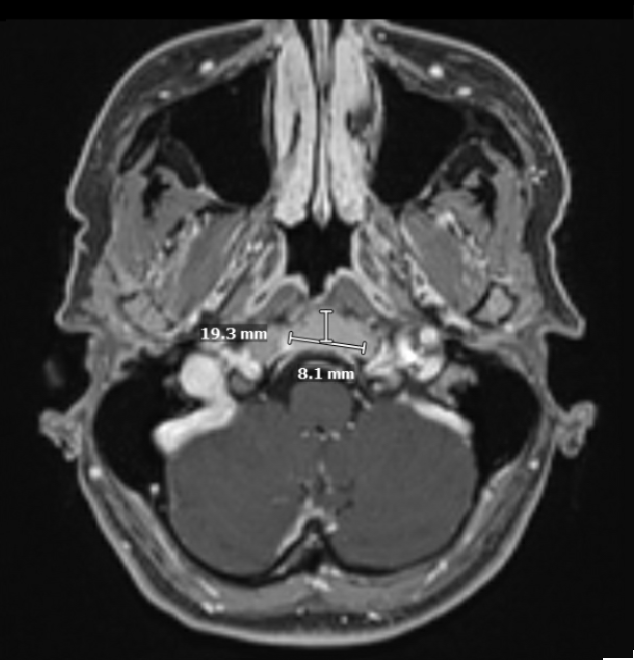
Case Presentation: A 49-year-old woman with epilepsy presented with progressive diffuse bone pain, chest and neck discomfort, and muscle spasms over several weeks. The pain was constant, aching, and most pronounced in the sternum, collar bones, and neck. Emergency department evaluation revealed diffuse osseous mottling on imaging and hypercalcemia. Laboratory studies demonstrated markedly elevated serum free kappa light chains (1,801 mg/L) with a highly abnormal kappa/lambda ratio (>100), raising concern for a plasma cell dyscrasia. CT and MRI imaging of the neck and skull base revealed multiple heterogeneous osseous lesions, including a 1.7 cm lesion in the left pterygoid process extending partially into the sphenoid sinus and a 1.9 cm lesion in the right thyroid cartilage, causing mild focal airway narrowing. Bone marrow biopsy demonstrated 50% cellularity with subtle interstitial plasma cell infiltrates. Fluorescence in situ hybridization analysis showed t(11;14) IGH::CCND1 fusion, gain of 1q, and gain of 16q. Biopsy of the thyroid cartilage lesion confirmed a plasma cell neoplasm, establishing the presence of Extramedullary Disease (EMD).
Discussion: EMD occurs in approximately 13% of multiple myeloma patients, with 7% at diagnosis and 6% during disease course [2,5]. The most commonly reported locations include soft tissues surrounding the axial skeleton (85% of cases), as well as lymph nodes, liver, kidneys, lungs, and skin [5]. In contrast, thyroid cartilage involvement is exceptionally rare, with only a small number of published cases frequently presenting with airway symptoms or with extension toward adjacent craniofacial structures [3,6]. EMD occurs when malignant plasma cells acquire the ability to proliferate outside the bone marrow niche through loss of adhesion molecules and increased expression of matrix metalloproteinases [7,8,16]. The patient’s cytogenetics represent a biologically complex subgroup. The t(11;14) translocation is generally considered a standard-risk abnormality with relative sensitivity to venetoclax [9,16,17]. However, gain of 1q is a well-established adverse prognostic feature linked to increased proliferation and resistance to proteasome inhibitors [9,10]. The coexistence of 1q gain with t(11;14) has been reported to worsen prognosis in some cohorts [18]. The presence of EMD itself is a high-risk feature, and the gain of 1q in this context may have contributed to the observed extramedullary dissemination and aggressive presentation. Historically, EMD has been associated with inferior survival, even in the era of proteasome inhibitors and immunomodulatory drugs [7]. The advent of anti-CD38 monoclonal antibodies in quadruplet regimens has led to deeper and more durable responses [11,12]. Early autologous stem cell transplantation remains the standard of care for transplant-eligible patients [13,14]. For patients with t(11;14) and refractory or relapsed disease, venetoclax-based therapy may be considered given its selective BCL-2 inhibition and efficacy in this cytogenetic subset [15-18].
Conclusions: Extramedullary and skull base involvement in multiple myeloma are rare but clinically significant. This case underscores the importance of recognizing atypical presentations, obtaining biopsy confirmation of EMD, and rapidly initiating intensive therapy, such as quadruplet regimens followed by transplantation, to optimize outcomes for these high-risk patients.
.png)