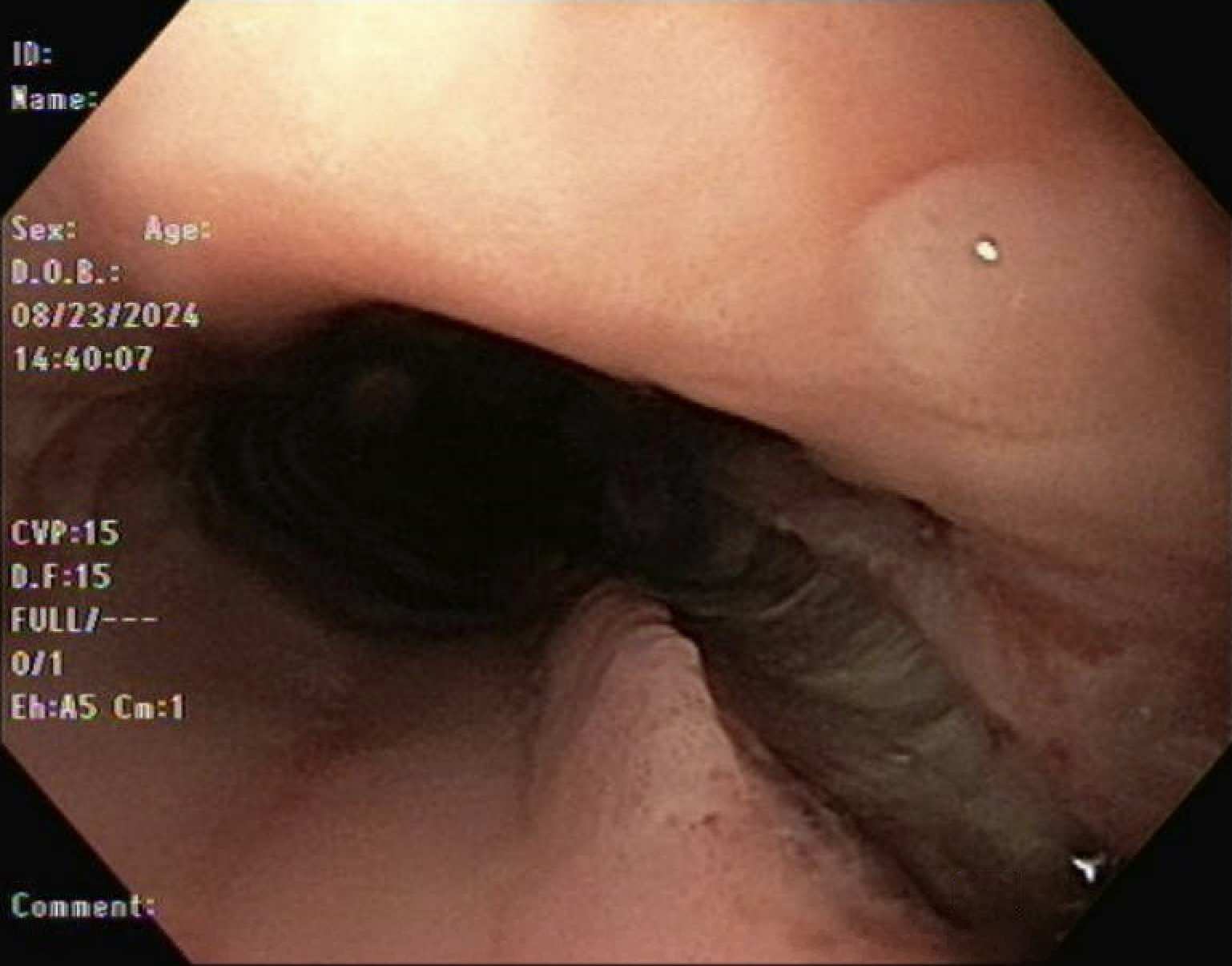
Case Presentation: A 48-year-old male with no significant past medical history presented with shortness of breath and midsternal chest pain after eating a bagel. Patient reported a globus sensation in his esophagus followed by multiple episodes of forceful retching prior to arrival. The patient denied a previous history of dysphagia or gastroesophageal reflux disease. In the emergency department, vital signs and physical examination were unremarkable except for mild epigastric tenderness. Initial laboratory values including CBC, CMP, and troponin were normal except for WBC of 17.2 bil/L without eosinophilia. Electrocardiogram and chest X-ray showed normal sinus rhythm and no acute abnormalities, respectively. The gastroenterology team was consulted and advised emergent esophagogastroduodenoscopy (EGD) for suspected food impaction. Endoscopy revealed multiple concentric rings and linear furrows, but no food bolus was observed; furthermore, a deep cratered, 15 cm linear tear was discovered in the esophagus, starting at a point 25 cm from the incisors and extending to the gastroesophageal junction (Figure 1). Due to the fear of perforation, no biopsy was taken, and the remainder of the procedure was aborted, prompting emergent thoracic surgery consultation to address the potential for transmural perforation. A CT scan with intravenous contrast showed a small pneumomediastinum but no esophageal perforation, and subsequent fluoroscopic esophagram confirmed no active leak but demonstrated narrowing and concentric rings with delayed emptying of the esophagus (Figure 2). The patient was managed conservatively and advised to continue a liquid diet for two weeks with outpatient follow up for EGD with biopsies.
Discussion: The risk of spontaneous esophageal injuries is well known in the context of eosinophilic esophagitis (EoE), particularly in patients experiencing episodes of retching which increases the risk of perforation, a rare but potentially life-threatening complication occurring in approximately 2% of cases [1,2]. Emerging data suggests that up to 50% of patients presenting with food impaction may have EoE [2]. Endoscopy in patients with EoE must be approached with caution due to the heightened risk of spontaneous or iatrogenic esophageal injury. Our case illustrates the importance of maintaining a high index of suspicion for spontaneous esophageal injuries in patients with unrecognized EoE. Currently, methods to reduce the risk of perforation during the pre-procedural period have not been clearly elucidated thereby raising the question of the role of pre-endoscopy chest CT or swallowed topical corticosteroids upon presentation for suspected food bolus obstruction. Further studies on pre-procedural management of adults with food impaction are needed to determine the optimal strategies to mitigate perforation risk in patients with undiagnosed EoE.
Conclusions: Spontaneous esophageal injuries are a recognized risk in patients with EoE, particularly during retching, which can lead to the rare but serious complication of perforation. With up to 50% of food impaction cases potentially linked to EoE, caution is essential during endoscopy due to heightened injury risks. Our case highlights the importance of vigilance for spontaneous injuries in unrecognized EoE. Currently, there is no clear guidance on reducing perforation risk prior to endoscopy, emphasizing the need for further research in the pre-endoscopy setting.