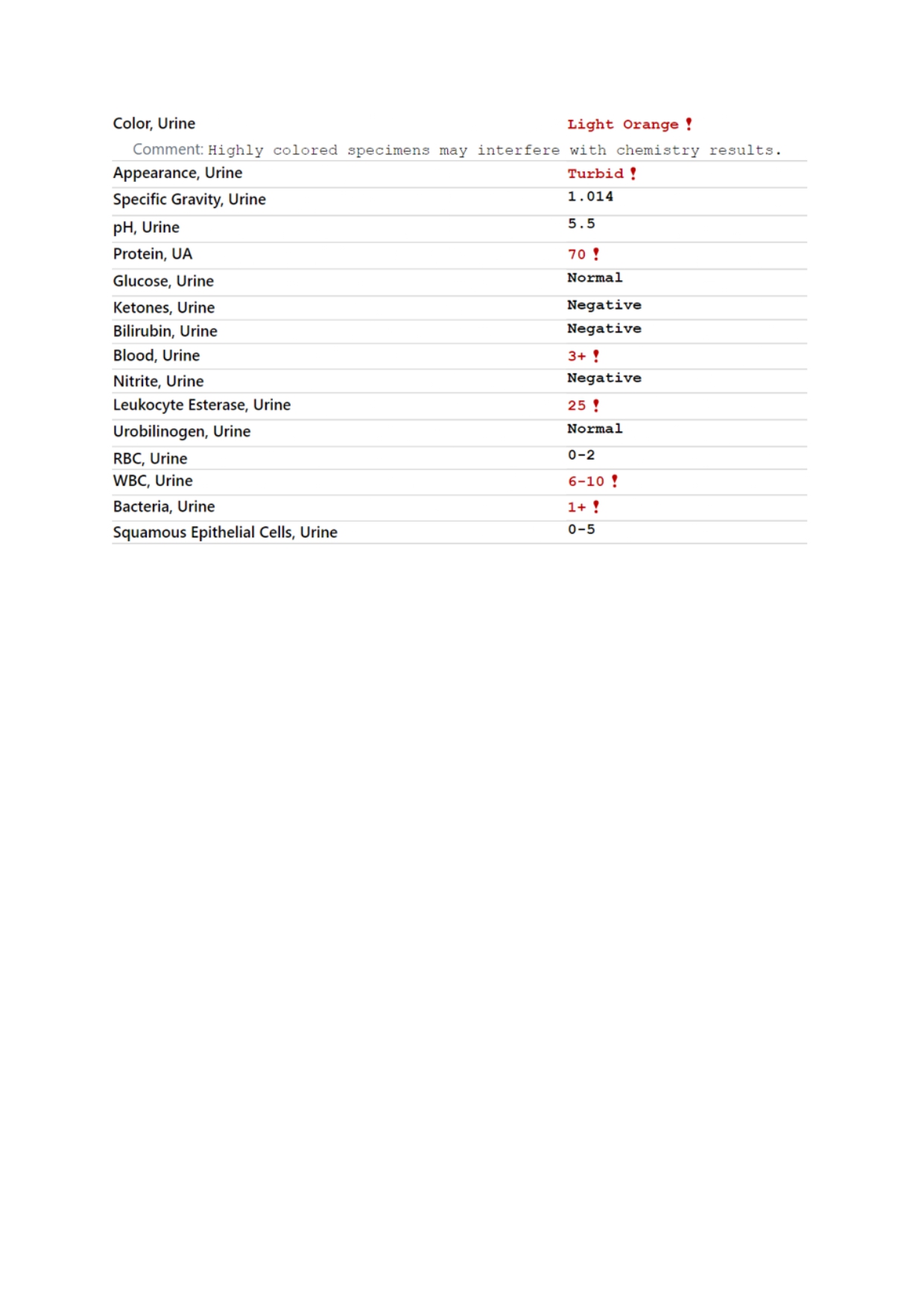
Case Presentation: A 91-year-old man with stable ischemic coronary artery disease presented with classic anginal chest pain relieved by nitroglycerin, initially suggesting acute coronary syndrome (ACS). Labs revealed elevated troponin I (353 ng/L), acute kidney injury (creatinine 2.54 mg/dL from baseline 1.3), and marked transaminitis (AST 506 U/L, ALT 369 U/L). ECG and imaging were non-revealing, and he was deemed not a candidate for left heart catheterization given advanced age, comorbidities, and clinical stability. Despite conservative management, intermittent chest discomfort persisted. A pivotal clue came from urinalysis positive for blood without RBCs, raising suspicion for rhabdomyolysis, later confirmed by a creatine kinase (CK) level >7000 U/L. Medication review revealed that the patient, on chronic atorvastatin therapy, had recently been started on Ranolazine as an adjunctive antianginal therapy, a CYP3A inhibitor that increases statin concentrations. Both agents were discontinued, and with aggressive IV hydration, his renal and hepatic indices improved, confirming the diagnosis and guiding recovery.
Discussion: Rhabdomyolysis can closely mimic acute coronary syndrome (ACS), particularly in elderly patients presenting with chest pain and elevated high-sensitivity troponin despite non-diagnostic ECGs. Although high-sensitivity troponin is cardiac-specific, modest elevations may occur in stable ischemic heart disease, renal dysfunction, or structural cardiac remodeling, complicating interpretation in multimorbid patients and sometimes prompting premature activation of ACS pathways.In this case, polypharmacy created the perfect storm: Ranolazine, a CYP3A inhibitor, was added to chronic statin therapy, leading to increased statin levels, skeletal muscle injury, and renal dysfunction that impaired clearance. The resulting muscle breakdown caused a marked creatine kinase rise, precipitating acute kidney injury and likely amplifying troponin elevation, further blurring the distinction between myocardial infarction and systemic muscle injury.The diagnostic breakthrough came not from advanced imaging but from a simple urinalysis showing heme positivity without red blood cells, an overlooked yet classic clue of rhabdomyolysis. Correlating this with rising creatine kinase and recent medication changes enabled early recognition and reversal of a potentially fatal cascade.This case highlights the hospitalist’s role as a diagnostic integrator; synthesizing pharmacologic, biochemical, and clinical data to navigate diagnostic ambiguity. Vigilance toward medication interactions, physiologic context, and evolving clinical findings, especially in elderly patients with comorbidities, can prevent unnecessary invasive procedures and medication-related harm. Such cases exemplify how attentive bedside reasoning continues to anchor the practice of high-value hospital medicine.
Conclusions: Rhabdomyolysis can masquerade as acute coronary syndrome, particularly in elderly patients with multimorbidity and polypharmacy. Recognizing laboratory discrepancies and medication interactions is key to avoiding unnecessary interventions. This case reminds us that diagnostic vigilance and not assumption, often makes the difference between misdiagnosis and meaningful recovery.
.jpg)