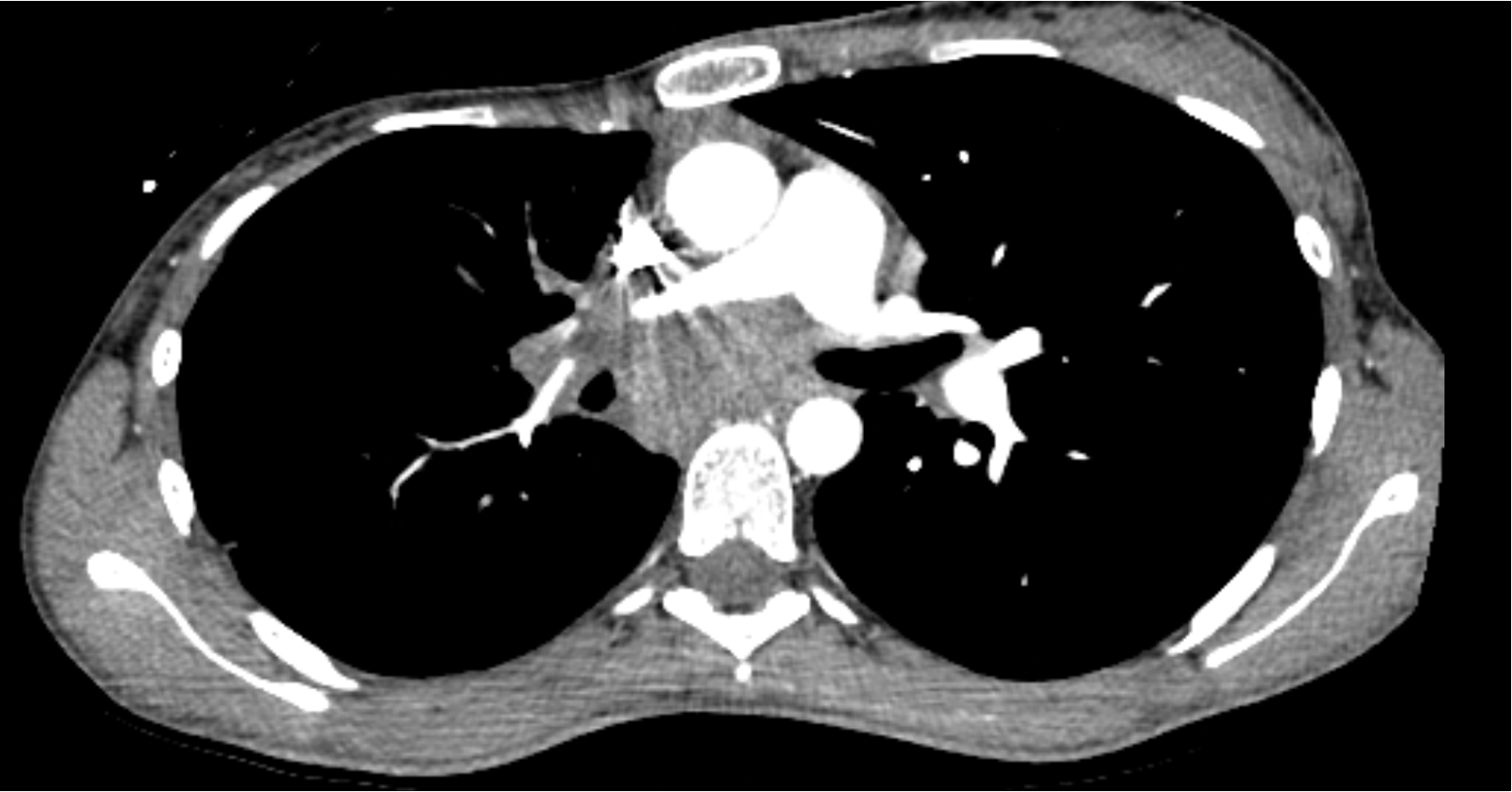
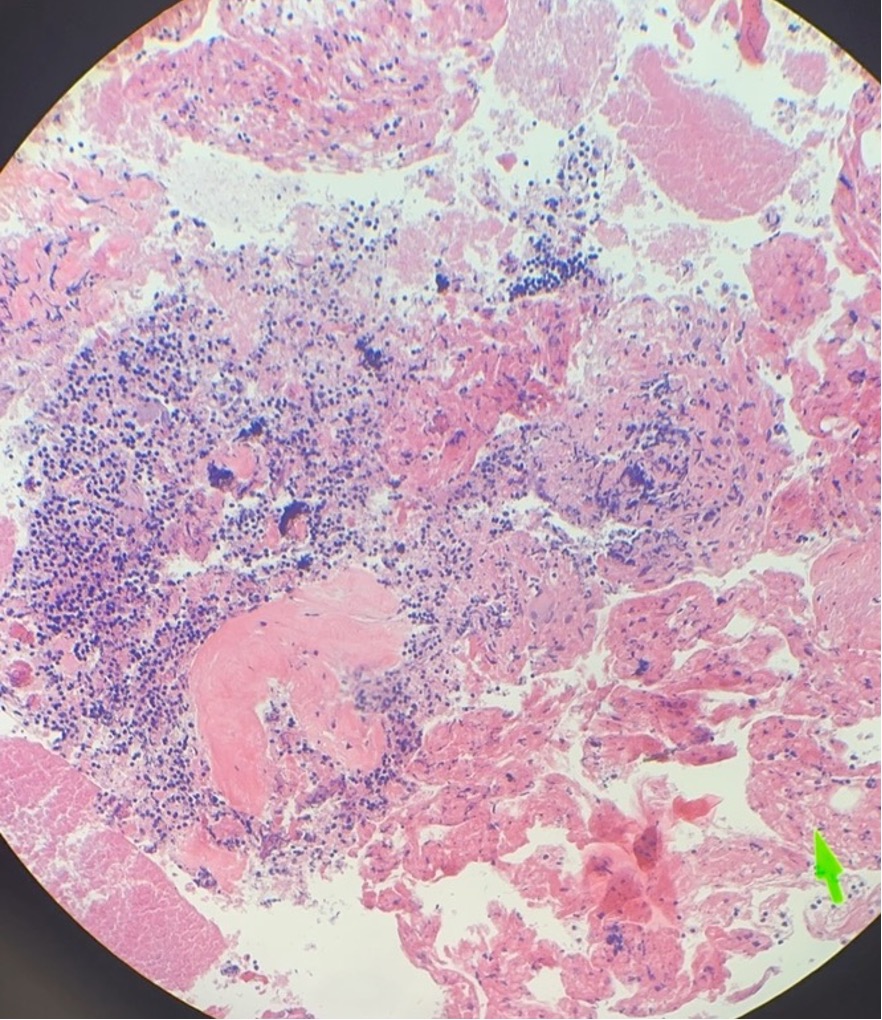
Case Presentation: A 22-year-old woman presented after an episode of syncope and chest pain. The patient reported weight loss and anorexia for 2 weeks and fever, fatigue, and chills for a few days prior to presentation. She had recently moved to Georgia from Missouri. She had no significant medical or family history. Initial workup showed a 4.5 cm sub-carinal mass encasing the pulmonary artery and causing pulmonary stenosis. Initial echocardiogram was normal, but she subsequently developed a moderate pericardial effusion during the next few weeks. Bronchoscopy with endobronchial biopsy (EBUS) was performed twice in addition to video-assisted thoracoscopic surgery with mediastinal biopsy of the mass and surrounding lymph nodes. Pathologic examination revealed necrotizing granulomatous inflammation with negative bacterial, fungal, AFB cultures, and negative cytology and flow cytometry.During the second bronchoscopy with EBUS, the patient was given 4 mg of dexamethasone pre-procedurally. Clinical improvement was noted for the next 24-48 hours. We hypothesized that dexamethasone decreased immune activation after suspected infection with histoplasmosis given her previous residence in Missouri. Itraconazole and prednisone were initiated to empirically treat for histoplasmosis. Around the time of treatment initiation, a urinalysis showed proteinuria and microscopic hematuria. Rheumatologic workup resulted cytoplasmic-antineutrophil cytoplasmic antibody (C-ANCA) positive with immunofixation titers of 1:320, serine proteinase 3 markedly positive at 640, and rheumatoid factor >200. Urinary sediment under phase contrast microscopy showed many red blood cells (RBC); 60% had dysmorphic features. During her hospital stay, the patient developed dermatologic manifestations including delayed pressure urticaria of the extremities that resolved with steroids and intermittent vasculitic rash in the lower extremities. With evidence of glomerulonephritis, vasculitic rash, and serologies positive for C-ANCA and serine proteinase-3 in the setting of necrotizing granulomatous inflammation, a primary diagnosis of GPA was made. Histoplasmosis with subsequent immune activation was considered in the diagnostic process, but GPA was favored as a diagnosis considering positive serologic testing and multiorgan manifestations. Itraconazole was discontinued with initiation of pulse dose steroids and rituximab. There was clinical improvement with initial steroid treatment including resolution of pericardial effusion as well as improvement of generalized symptoms. Subsequent evaluation of glomerulonephritis and mediastinal mass were planned for the outpatient setting.
Discussion: Granulomatosis with polyangiitis (GPA) is a C-ANCA necrotizing vasculitis with non-specific presenting clinical features of GPA commonly involving the sinuses, urinary tract, joints, and skin. Our 22-year-old female patient, who initially presented with a sub-carinal mass, had an unusual presentation of GPA. Previous cases of GPA have associations with necrotizing granulomatous masses. This is the first case we found to have GPA present as a sub-carinal mass with necrotizing granulomatous inflammation; subsequent imaging of the sub-carinal mass following treatment would be of particular interest.
Conclusions: GPA should be considered in the differential for masses with necrotizing granulomatous inflammation.