
Background:
Providing efficient, interdisciplinary care in academic centers today is greatly challenged by work‐hour restrictions, the resulting fragmented team structures, and frequent geographic discontinuity of physician teams. Our objective was to geographically localize physician teams to maximize rounding efficiency and promote inter‐professional communication.
Methods:
Our teaching service admissions were restructured from admitting to 8 different wards in 2 hospital towers to stationing each teaching team on 1 floor. One overflow floor was shared by all medicine teams. Nurse participation in bedside attending rounds was encouraged. To assess the effect of geographically locating our teams on staff perceptions of communication and efficiency, surveys were provided to attendings, residents, nursing, social work, utilization management, and physical/occupational therapy on the medicine teaching services pre‐ and postimplementation of geographic rounding. All analyses were performed using chi‐square tests.
Results:
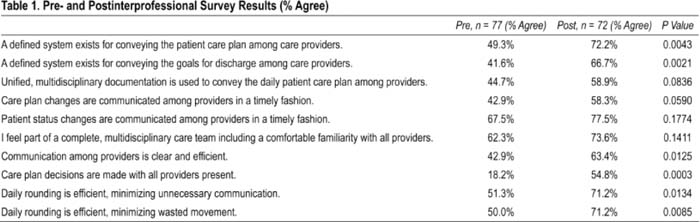
Survey data showed significant improvement in the structure, efficiency, and communication of the interprofessional care teams after implementation of geographic rounding (Table 1).
Conclusions:
Geographic restructuring of our teaching services created a rounding infrastructure that promoted face‐to‐face bedside communication on the interprofessional care team. This significantly improved communication of both the daily care plan and discharge goals among providers. We also found that our staff believed both communication and movement efficiency was markedly improved. It is still undetermined whether these perceived gains lead to improved quality of patient care or house staff education.
Author Disclosure:
D. Mancini, none; R. Albert, none; S. Chadaga, none; K. Heist, none; A. Keniston, none; K. Heade, none; E. Chu, none.