Background:
Red blood cell (RBC) transfusion is a common procedure in hospitals, with approximately 14 million units transfused in the U.S. in 2011. Although direct transmission of infectious agents via allogeneic RBC transfusion is now quite low, transfusion‐related immunomodulation has been associated with an increased risk of infection. Leukoreduction of RBCs, which is done for 85% of units in the U.S., may ameliorate immunomodulation, but other practices such as lowering hemoglobin thresholds for RBC transfusions limit patients’ exposure to blood products. We evaluated the current evidence from randomized trials regarding restrictive transfusion thresholds and the effects on infections.
Methods:
We conducted a systematic review and meta‐analysis of the randomized trials which incorporated two comparator arms – restrictive versus liberal RBC transfusion strategies – to evaluate their impact on the incidence of healthcare‐associated infection. MEDLINE, Embase, Web of Science, Cochrane Register of Controlled Trials, ClinicalTrials.gov, International Clinical Trials Registry Platform, and the ISRCTN registry were searched through 8/23/2013. Random effects models were used to pool risk ratios and risk differences across studies.
Results:
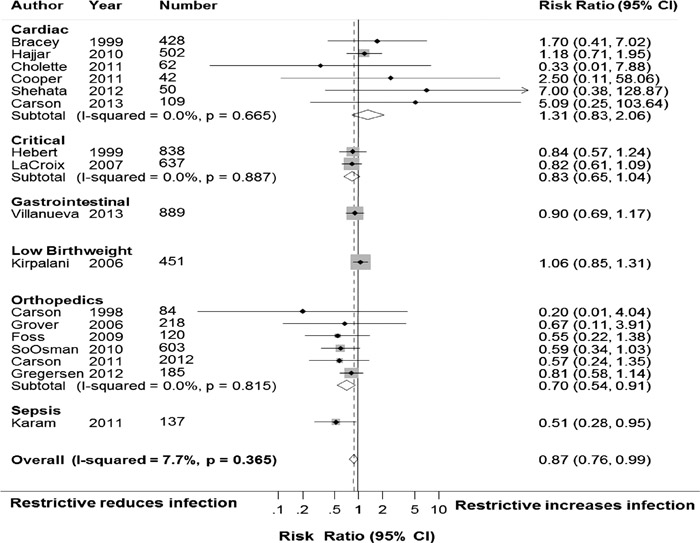
A total of 18 trials with 8037 patients met criteria, of which 17 trials (n=7486 patients) contained sufficient information for meta‐analyses. Restrictive RBC transfusion strategies decreased the risk of infection by 18% (95% CI: 5% to 28%) with little heterogeneity (I2 = 0.0%; τ2<0.0001). Pooled risk of infection was 11.8% in the restrictive group and 16.9% in the liberal group. The number needed to treat with restrictive strategies to prevent infection was 34 (95% CI, 21 to 110) and the number of avoided infections per 1000 patients was 29.6 (95% CI, 9.1 to 47.5). Leukoreduction of RBC units did not mitigate the effect of a liberal transfusion strategy on infection. With stratification by patient type, there was a 30% decreased risk of infection with restrictive RBC use (95% CI, 9% to 46%) in orthopedic patients which yielded $1.6 to $2.0 billion estimated cost savings to U.S. hospitals annually. Patients with sepsis exhibited a 49% decreased risk of nosocomial infection with lower RBC thresholds (95% CI, 5% to 72%). There were no significant differences in the incidence of infection by RBC threshold for patients with cardiac disease or acute upper gastrointestinal bleeding, the critically ill, or for low birth‐weight infants.
Conclusions:
Restrictive RBC transfusion strategies are particularly beneficial in patients undergoing hip or knee arthroplasty and in patients with sepsis. Implementing restrictive strategies would likely decrease the incidence of healthcare‐associated infection and reduce healthcare costs.