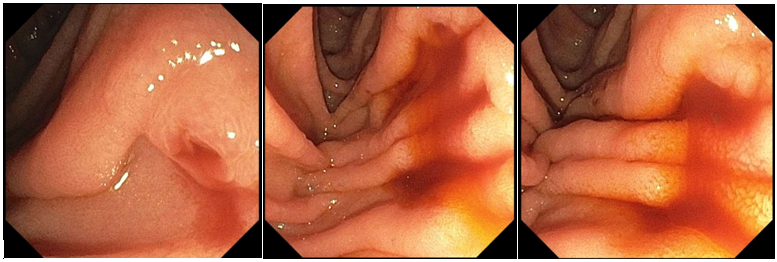
Case Presentation: A 34-year-old male presented with several months of intermittent melena and progressive weakness. He denied fevers, abdominal pain, nausea, vomiting, or dyspnea. Physical exam showed tachycardia and pallor. Laboratory evaluation revealed hemoglobin 1.5, MCV 80, platelets 560, INR 1.5, and lipase 94. Further workup showed a component of iron deficiency anemia and appropriately elevated reticulocyte count, but normal haptoglobin, folate, and vitamin B12 levels. Computed tomography angiography (CTA) of the abdomen and pelvis revealed no acute GI bleed but demonstrated hepatic cirrhosis with splenomegaly. Magnetic resonance cholangiopancreatography (MRCP) revealed acute pancreatitis with a 2 cm necrotic cystic collection in the pancreatic head. Colonoscopy was unremarkable, but an upper endoscopy using a side-viewing duodenoscope revealed red blood emanating from the major papilla, confirming hemosuccus pancreaticus (HP) as the bleeding source. Given the high clinical suspicion for a pancreatic arterial source, Interventional Radiology was consulted who performed a prophylactic embolization of the gastroduodenal artery. The patient’s hemoglobin subsequently improved and no further bleeding occurred during his hospitalization.
Discussion: Hemosuccus pancreaticus is a rare but life-threatening cause of upper gastrointestinal (GI) bleeding, often missed due to its intermittent nature and subtle imaging findings. Diagnosis typically requires high clinical suspicion and collaboration between hospitalists and multiple specialists. CTA can be negative due to episodic bleeding, emphasizing the importance of advocating for repeated or alternative imaging when the clinical picture remains concerning. Endoscopy was pivotal in our case, as visualization of blood from the major papilla is the hallmark of HP. Side-viewing duodenoscopy greatly increases diagnostic yield (70.1% vs 29.6% for standard forward-viewing endoscopy) and should be requested by hospitalists when suspicion remains despite nondiagnostic initial studies [3].In addition, transcatheter arterial embolization offers a safe, minimally invasive alternative to surgery [1, 2]. In this patient, the decision to proceed with gastroduodenal artery embolization despite unremarkable imaging suggests that in high-risk cases where the clinical and endoscopic findings point towards an arterial pancreatic source, prophylactic embolization may be justified. From a hospital medicine perspective, early consultation with Interventional Radiology is crucial, as prompt collaboration can prevent recurrent bleeding, minimize transfusion requirements, and expedite definitive therapy.Lastly, the medicine team constantly explored alternative causes of the patient’s symptoms, recognizing that while definitive interventions often rest with specialists, hospitalists are vital in maintaining diagnostic momentum.
Conclusions: Hemosuccus pancreaticus is an uncommon but critical diagnosis for hospitalists to consider in patients with unexplained or recurrent upper GI bleeding, particularly in patients with pancreatitis or pancreatic cysts. Ultimately, this case not only highlights the diagnostic difficulty and successful management of HP, but it also emphasizes the hospitalist’s key role in recognizing rare causes of GI bleeding, ensuring timely multidisciplinary engagement, and advocating for tailored diagnostic strategies when standard evaluations fail.