Background:
Aspirin (ASA) resistance and high mean platelet volume (MPV) are associated with increased risk for cardiovascular events. However, a relationship between high MPV and aspirin resistance, as measured by platelet aggregation, has not been reported. Our aim was to examine whether individuals with high MPV are more likely to have aspirin resistance.
Methods:
Fasting blood samples were obtained from healthy participants (n = 2363 from 584 families) with a family history of premature coronary artery disease. Optical aggregation was measured in platelet‐rich plasma after samples were stimulated with collagen (2 and 5 μg/mL), ADP (2 and 10 μmol/L), or arachidonic acid (1.6 mmol/L) before and after 14 days of ASA therapy. For each dose of each agonist, we examined the association between MPV and aspirin resistance separately. Individuals with any arachidonic acid–mediated aggregation were defined as aspirin resistant. For collagen and ADP, individuals in the highest quartile of aggregation after ASA therapy were defined as aspirin resistant. We used logistic regression with adjustment for familial relationship.
Results:
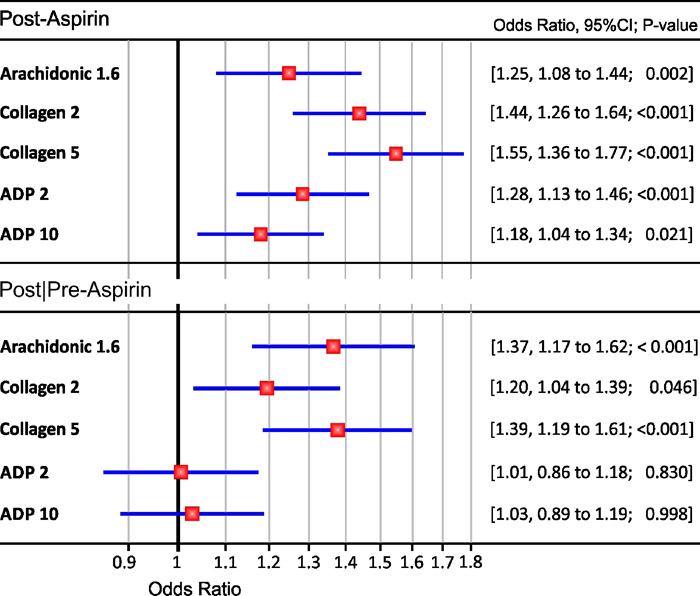
Mean (SD) age was 45.9 (13.5) years; 55% were female; 40% African American; 25% current smokers, 37% hypertensive, and 12% diabetic. In unadjusted analysis, MPV was associated with aspirin resistance as defined by each agonist and dose. This association remained significant after adjusting for age, sex, race, hypertension, diabetes, low‐density lipoprotein cholesterol, smoking status, and fibrinogen (Figure, upper). After adjusting for agonist‐specific pre‐ASA platelet aggregation (Figure, lower), MPV remained associated with aspirin resistance as defined by collagen and arachidonic acid but was no longer associated with ADP‐defined aspirin resistance.
Conclusions:
High MPV, commonly due to younger and more aggregable platelets, is associated with arachidonic acid– and collagen‐defined aspirin resistance independent of cardiovascular risk factors and native platelet reactivity. Our findings may provide interesting insight into the effect of platelet life span and turnover on aspirin resistance.