Background: High-value care (HVC) is an increasingly important component of medical education. This study aimed to assess differences in medical students’ perceptions and behaviors towards HVC during surgical versus non-surgical rotations and to evaluate the impact of an educational first-year HVC course on these outcomes.
Methods: A cross-sectional, annual survey was administered from 2021-2024 to medical students who completed surgical (n=120) and non-surgical (n=237) rotations. Surgical included OBGYN and surgery rotations while non-surgical encompassed pediatrics, internal medicine, emergency medicine, psychiatry, and neurology. The survey assessed key HVC components such as transparency of cost, barriers to HVC practice, comfort in discussing HVC, perceived receptiveness to HVC discussions, and frequency of excessive testing. Responses were compared between surgical and non-surgical rotations using Wilcoxon rank sum tests with bootstrapping for median and 95% confidence intervals (CI). The impact of a first-year HVC course was evaluated by comparing outcomes between students who took the course (surgical: n=59, non-surgical: n=109) and those who did not (surgical: n=61, non-surgical: n=128).
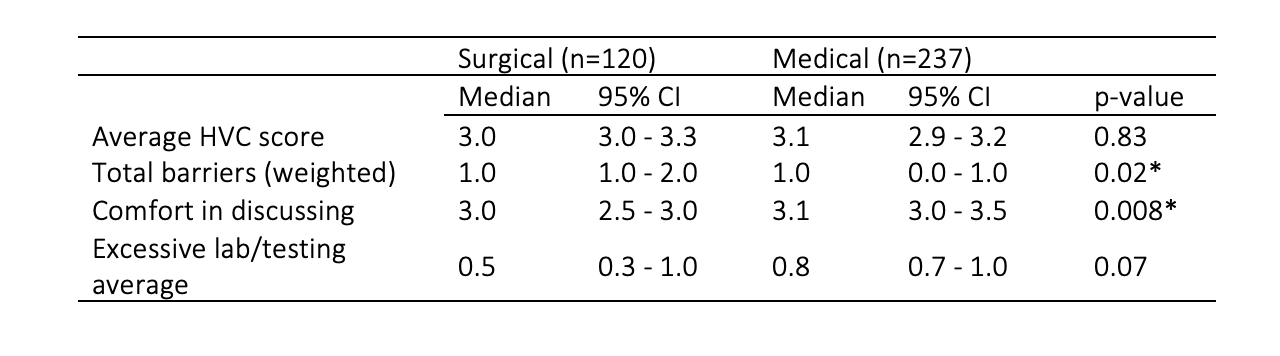
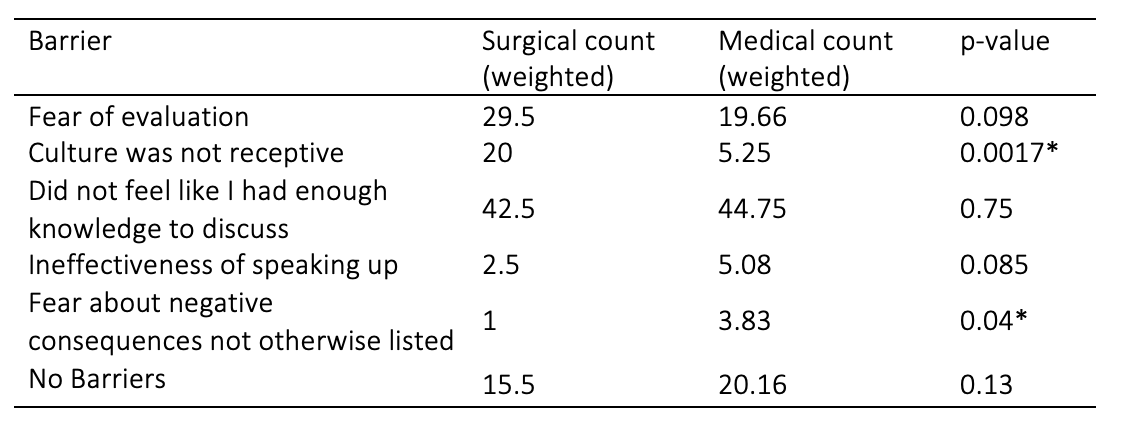
Results: Overall, there were no significant differences in a composite HVC score between surgical and non-surgical rotations that assessed for unnecessary testing, discussions of cost, ability to voice concerns about HVC, and prioritization of HVC practices (median 3.0, 95% CI: 3.0-3.3 vs 3.1, 95% CI: 2.9-3.2, p=0.83). However, students reported more barriers to HVC practice in surgical rotations (median 1.0, 95% CI: 1.0-2.0 vs 1.0, 95% CI: 0.0-1.0, p=0.02) and felt less comfortable discussing HVC (median 3.0, 95% CI: 2.5-3.0 vs 3.1, 95% CI: 3.0-3.5, p=0.008) than in non-surgical rotations. The most common barrier in both rotations was feeling a lack of knowledge to discuss HVC (surgery: 42.5, non-surgical: 44.75, p=0.75). Students perceived the culture as less receptive to HVC in surgical rotations compared to non-surgical rotations (20.0 vs 5.25, p=0.0017). There were no significant differences in HVC outcomes between those who took the first-year course and those who did not.
Conclusions: While overall HVC scores were similar between surgical and non-surgical rotations, students faced more barriers and felt less comfortable discussing HVC in surgical settings. The first-year HVC course showed mixed effects on outcomes, with trends towards improvement in some areas but without any significant differences. These findings highlight the need to address barriers to effective HVC education in surgical clerkships and suggest potential benefits of early HVC training for students irrespective of specialty. Future research should explore strategies to enhance students’ confidence in applying HVC principles across different clinical settings.