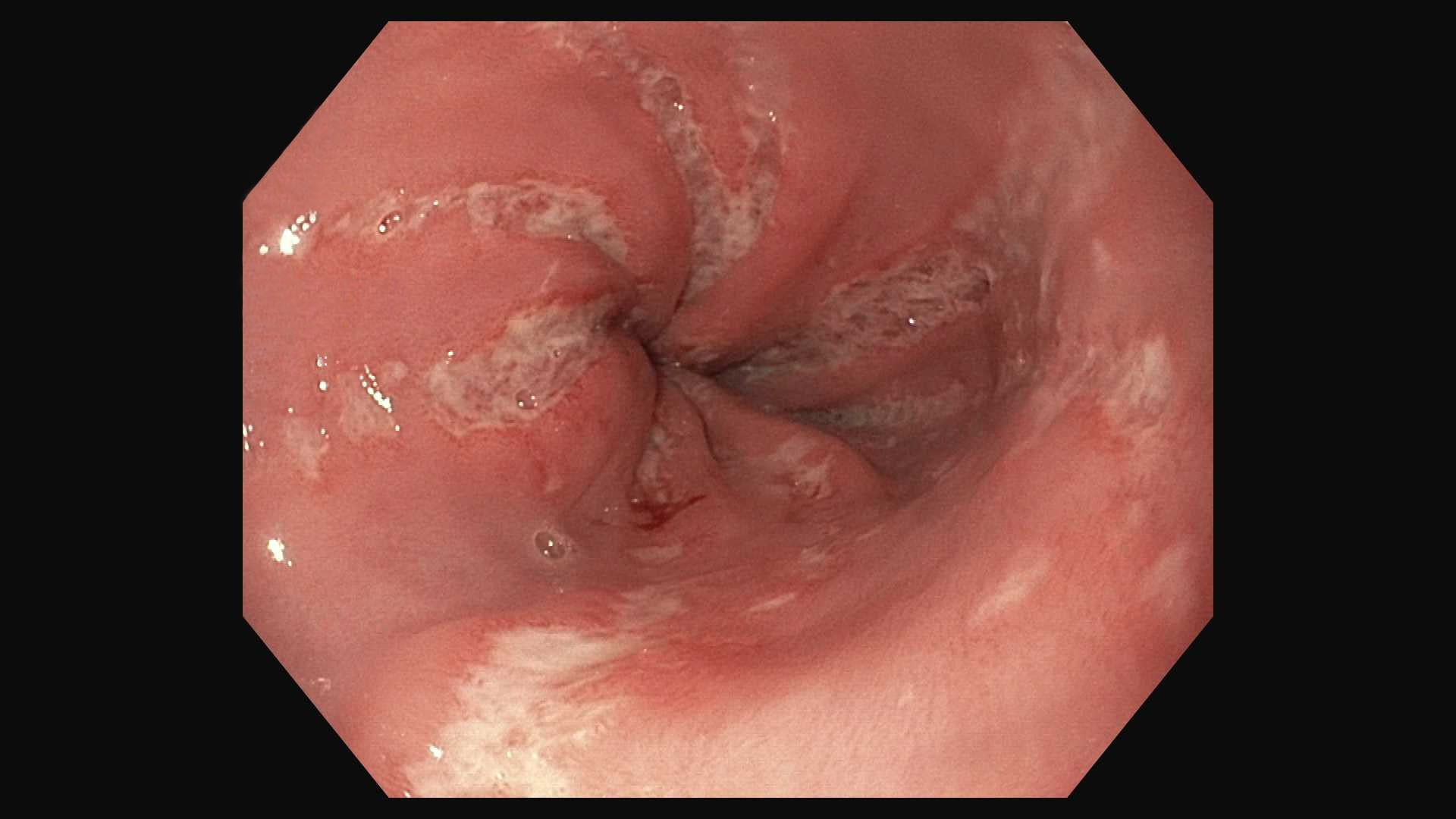
Case Presentation: A 22-year-old male with no medical history presented to the emergency department with a 4-day history of fevers and odynophagia which progressively prevented intake of solids and liquids. He reported associated shortness of breath with pleuritic chest pain. He appeared nontoxic with sputum collecting in a bedside cup. He had a fever of 101F and was tachycardic at 110. The rest of the exam was unremarkable. Labs revealed a creatinine of 1.5 and a D-dimer of 595. CT angiogram of the chest showed no evidence of pulmonary embolism but noted abnormal circumferential distal esophageal thickening. An EGD was performed and revealed severe esophagitis with punctate esophageal ulcerations, linear ulcers, and linear gastric erosions. HIV, EBV, CMV and HSV tested negative. The fevers subsided, the tachycardia improved with IV hydration and his creatinine decreased to 1.2.Upon further questioning, it was discovered that the patient was a competitive weightlifter and often ingested pre-workout supplement powder. Normally, this caffeine rich powder is diluted in liquid and ingested prior to weightlifting. In the week leading up to his admission, he had run out of the solvent he normally used to dissolve the powder and had begun “dry-scooping”. The patient explained that he put a dry scoop of powder (8 grams per scoop) directly into his mouth and would swallow it with a sip of water. The patient noted that the powder was not completely dissolved when swallowing, and pockets of dry powder was ingested. He did this thirty minutes before exercising 3-4 times per week for two weeks prior to admission. The powder he reported using had ingredients that included L-citrulline, Beta-alanine, malic acid, sodium citrate, citric acid, and tartaric acid. “Dry-scooping” causing mucosal injury leading to esophageal ulcers is the most plausible etiology. The pathology report described basal cell hyperplasia, focally increased intraepithelial eosinophils (up to 15 cells/hpf) and superficial erosions with fibrinous exudate on the surface. The sample was negative for goblet cells. It is likely that these findings represent damage done to the esophageal mucosa from “dry-scooping” of pre-workout powder. Counseling against this increasingly popular practice was provided. The patient was initiated on a proton pump inhibitor for 2 weeks with progressive improvement in his symptoms noted after the first week.
Discussion: Recently, “dry-scooping” of pre-workout supplements has become a trend that has gained traction on social media platforms such as TikTok. These products are poorly regulated in the US and may contain toxic ingredients. Pre-workout powder is a supplement used by athletes, body builders and fitness enthusiasts that is rich in caffeine and other ingredients to increase energy and performance of the user. There are numerous news reports of adverse reactions from dry scooping, most describing the overconsumption of pre-workout powder and its effects primarily linked to caffeine content. There is very little scientific literature published about the harmful effects of dry scooping itself and none describing dry scooping as a cause of caustic ingestion.
Conclusions: In this case, we have proposed “dry-scooping”, to be the cause of a case of odynophagia and esophageal ulcerations. Effort should be taken to combat the popular trend on the internet and to educate our patients on the dangers of “dry-scooping”. Providers should consider inquiring about “dry-scooping” when faced with unexplained cases of esophagitis.