Background: Michigan Medicine’s Hospital Care at Home (HCAH) Program was designed to provide eligible patients living in Southeast Michigan hospital level care from their own homes. Since the advent of the CMS Hospital at Home Waiver in Nov 2020, 93% of HCAH programs have been in urban locations, with prominent programs in cities such as Boston, Baltimore, and New York City. The Michigan Medicine HCAH program is unique from other Hospital at Home programs in its service area, caring for a range of patients in more suburban and rural locations and with a larger Geriatric population.
Methods: Eligible patients were admitted from the Emergency Department (ED) or transferred from an in-hospital inpatient or observation unit. A small subset of patients were admitted directly from home. Traveling nurses visited patients twice daily, and physicians visited in-home once per day. According to the 2020 Census Bureau Urban Area classification, the cities of Ann Arbor, Chelsea, Dexter, Milan, and South Lyon are designated as urban areas. Any area not within these cities qualify as rural.
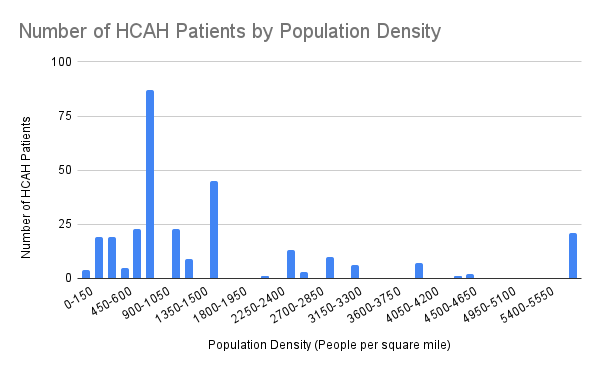
Results: The median age of admitted patients in this time period was 71.05 years old with a standard deviation of 17.37 years. 138 out of 298 total patients resided in urban areas, and 134 patients resided in rural areas according to census designations. By population density metrics alone, 157 patients resided in an area with a population density less than 1000 people per square mile. Out of 327 total HCAH enrollments, 60 (18.3%) resulted in a 30 day post-discharge ED visit. 44 enrollments resulted in a 30-day hospital readmission, either inpatient or outpatient, resulting in 13.4% 30-day hospital readmission rate. In patients living in census-designated urban areas, 31 out of 150 (20.67%) enrollments resulted in 30-day ED visits and 20 visits resulted in hospital readmissions (13.3%). In rural areas, 29 out of 177 (16.38%) visits result in ED visits, and 24 (13.56%) resulted in hospital readmissions. In a two-proportion z-test, no significant differences were found in rates between ED visits nor with readmissions for HCAH patients from urban and rural areas. During December 2021 to January 2024, all hospital ED utilization rates were 14.2%, and all hospital readmission rates were 12.4%. When comparing rates of followup ED visits in a two-proportion z-test, there was a significant increase (p = 0.03318) in hospital readmissions for HCAH compared to all hospital admissions. However, no significant difference was found between the two in ED utilization.
Conclusions: A large majority of Hospital at Home programs offering inpatient-level services do so in primarily urban areas, resulting in a disparity in rural healthcare access. The Michigan Medicine HCAH Program received a roughly equal mix of patients residing in rural and urban settings, and saw similar ED utilization rates in rural HCAH patients compared to urban HCAH patients. There was an increase in hospital readmissions for patients in our HCAH program compared to all hospital admissions, indicating there are areas for improvement in tailoring HCAH to more rural populations.