Background: The electronic health record (EHR) is a major focus of a hospitalist’s daily work but is also often a frustration. Organizations offer providers the chance to recommend improvements to the system, but frequently there are significant delays in implementation or the request does not even cross the threshold for institutional action. Additionally, of those projects that are approved, the build design is not always user-oriented and often falls short of what the users expect, despite significant back-and-forth communication between the requester and IT analysts. There is an opportunity provided by some EHR vendors for physicians to receive extra training to directly modify the EHR with only minimal institutional resource requirement (1). This provider builder program requires significant time commitments and may only be offered to a handful of provider champions. Hospitalists, with the holistic view of patient care processes, the flexible work schedule to accommodate training sessions, and the deep, direct interaction with the EHR, are uniquely positioned to be the ideal provider group to take advantage of this opportunity.
Purpose: The aim of our project was to create an opportunity for multiple hospitalists to obtain the necessary training to become certified to modify the EHR and evaluate the potential impact within our hospitalist group.
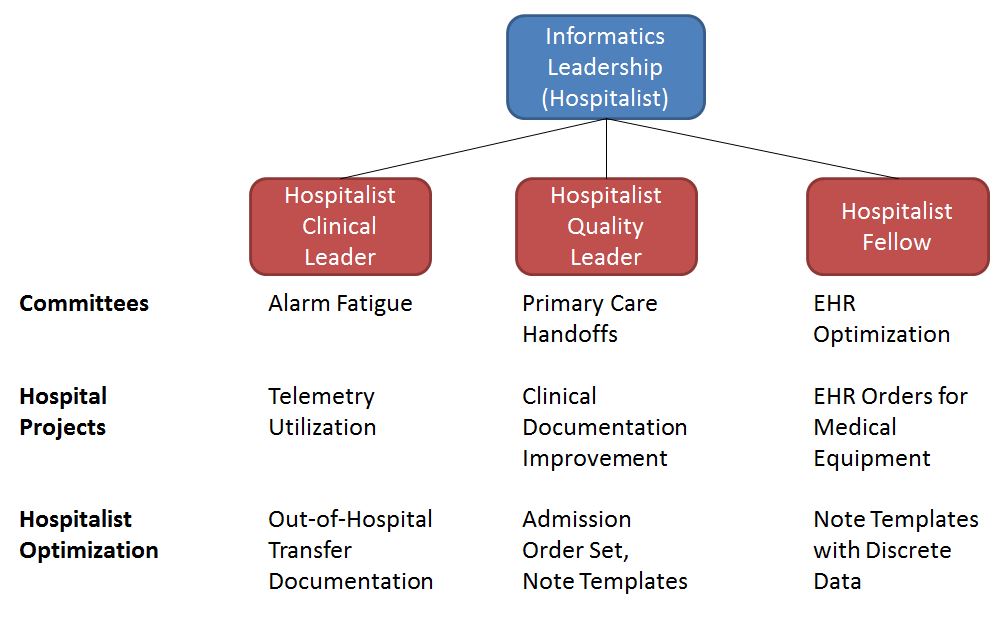
Description: The study institution is a large, academic, urban, tertiary referral center that currently uses Epic (EpicCare, Verona, WI) as its sole EHR. At the time of the project start, the hospitalist group had over 40 providers and cared for the largest volume of patients among all provider groups in the institution. Primary training in EHR modification was offered onsite in August 2018 and invitations were given to two attending hospitalists and one hospitalist fellow. An additional hospitalist had previously completed the training and holds an informatics leadership position in the institution. After completion of the initial course, providers were given access to EHR modification tools and were allowed to submit project proposals via an expedited review pathway. To complete the certification process, the providers completed a second training course at the vendor’s facility. Since completion of training, the hospitalist EHR builder team has led the implementation of three major projects: 1. Appropriate telemetry utilization order update and electronic alert, 2. Transfer of care note with embedded data elements, 3. Admission order set fit to hospitalists workflow and patients populations with updated venous thromboembolism prophylaxis module. The quantitative impact of each of these interventions is still being measured, but the feedback from hospitalist providers and leadership has been strongly positive. An additional benefit to the providers competing the advanced training has been their ability to serve as a technical expert, as well as a clinical expert, in the institution to drive innovative EHR interventions that are user-friendly and system-compatible. This has increased the hospitalist voice within the institution as the providers have been asked to serve on multiple institutional committees, and the hospital medicine group overall has been recommended to pilot a variable of EHR improvements (Figure 1).
Conclusions: Training multiple providers within a single hospitalist group to modify the EHR is feasible and can lead to significantly faster implementation of formal EHR changes and increase hospitalist visibility within the institution.