
Background:
Hospitalists must help find innovative solutions to challenging problems that face hospitals today. Hospitals face a physician shortage for both hospitalists and other specialty physicians. And hospitals face falling revenues and are under intense pressure to cut costs. Telemedicine has seen dramatic leaps in capability recently and has the potential to help resolve these challenges. The concept of “remote presence” has developed, where a physician can transmit via state‐of‐the‐art mobile telemedicine, a level of personal interaction previously unachievable. This study evaluated hospitalists' ability to perform initial patient admissions (the history and physical) utilizing the InTouch Health RP‐7 telemedicine platform equipped with an electronic stethoscope, The RP‐7 has been shown to be useful for stroke evaluations in the emergency department (ED), for in‐hospital rapid response, and for critical care rounding on patients.
Methods:
Hospitalist‐based telemedicine admissions was assessed with a prospective study comparing a study group of patients admitted via telemedicine and a control group admitted in person. All patients presenting to the ED were eligible except for critical care admissions and patients with altered mental status. Times studies were used to evaluate the efficiency of admissions. Surveys of patients, hospitalists, ED physicians and nurses, and extenders (assistant for the physicals) were gathered to assess satisfaction. Hospital length of stay (LOS) was measured. Compliance with history and physical dictation, order set usage, medication reconciliation, and DVT prophylaxis were obtained. Where possible, results of groups were compared using the unpaired t test.
Results:
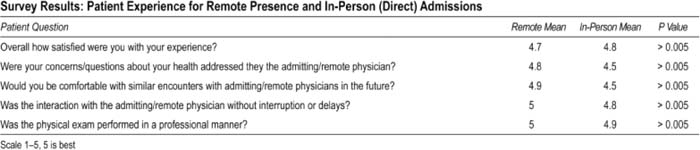
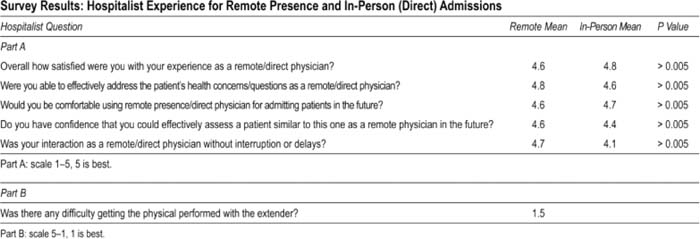
Twenty‐two patients were admitted by remote presence, with 10 patients admitted in person. The total time taken to perform remote (51 minutes) and in person (50 minutes) admissions was comparable (P > 0.005). Surveys of patients, hospitalists, and ED physicians and extenders indicated an excellent experience with remote presence admissions. ED nurses had a very good experience but revealed a privacy concern not specific to remote presence (noise transmission in ED rooms separated only by curtains). Hospital metrics were similar, including LOS, order set compliance, history and physical dictation, and DVT prophylaxis
Conclusions:
Hospitalists using remote presence can perform admissions in the ED. A hospitalist using telemedicine can now reach offsite locations, offer night coverage solutions, and complement other hospital telemedicine services. Mechanisms must be in place for in‐house backup.
Author Disclosure:
K. Godamunne, Eagle Hospital Physicians, employee.