Background: The management of hospitalized patients is becoming increasingly complex due to aging population, rise in multimorbidity, polypharmacy, and the increasing fragmentation of care systems¹. At the same time, inpatient bed occupancy rates in the US are projected to reach 85% as early as 2032² and patient safety events remain stubbornly high. Given these pressures, hospitalists rely on prompt and high-quality subspecialty consultations to ensure safe and timely patient care. Hospitalists’ perception of common challenges associated with subspeciality consultation can therefore be a valuable tool to guide system improvement efforts to optimize the consultation process.
Methods: We conducted a qualitative study of providers’ perception of the consultation process at our 1000-bed academic safety-net Institution. An online survey was sent to all hospitalist and emergency department providers. Participation was voluntary and responses were kept confidential. Respondents were asked to rate and comment on consultant promptness, quality of recommendations received and appropriateness of follow up after initial consultation. A 5-point Likert scale was used for the rating, while a dedicated space was provided for comments in free text. Thematic analysis approach was used to analyze comments. Open, line-by-line coding was performed by the two primary authors (GA and GK). Codes were combined using the techniques of constant comparison and axial coding to generate key categories in an inductive fashion. Categories were grouped together to generate themes and subthemes by senior author AS. Categories that did not explicate a particular point of view were subsumed into other categories. Any conflict about assignment of codes was resolved by discussion and mutual agreement.
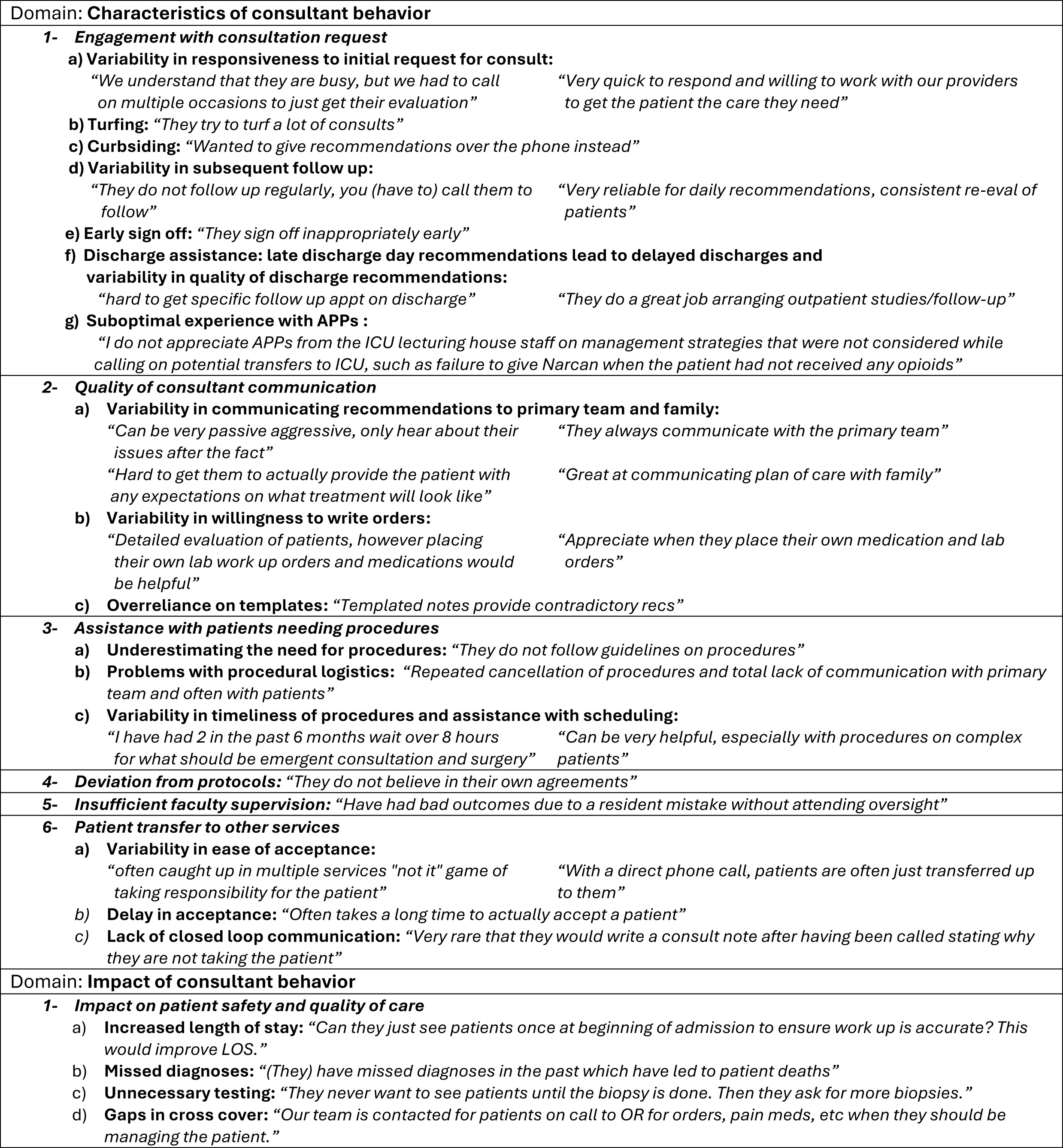
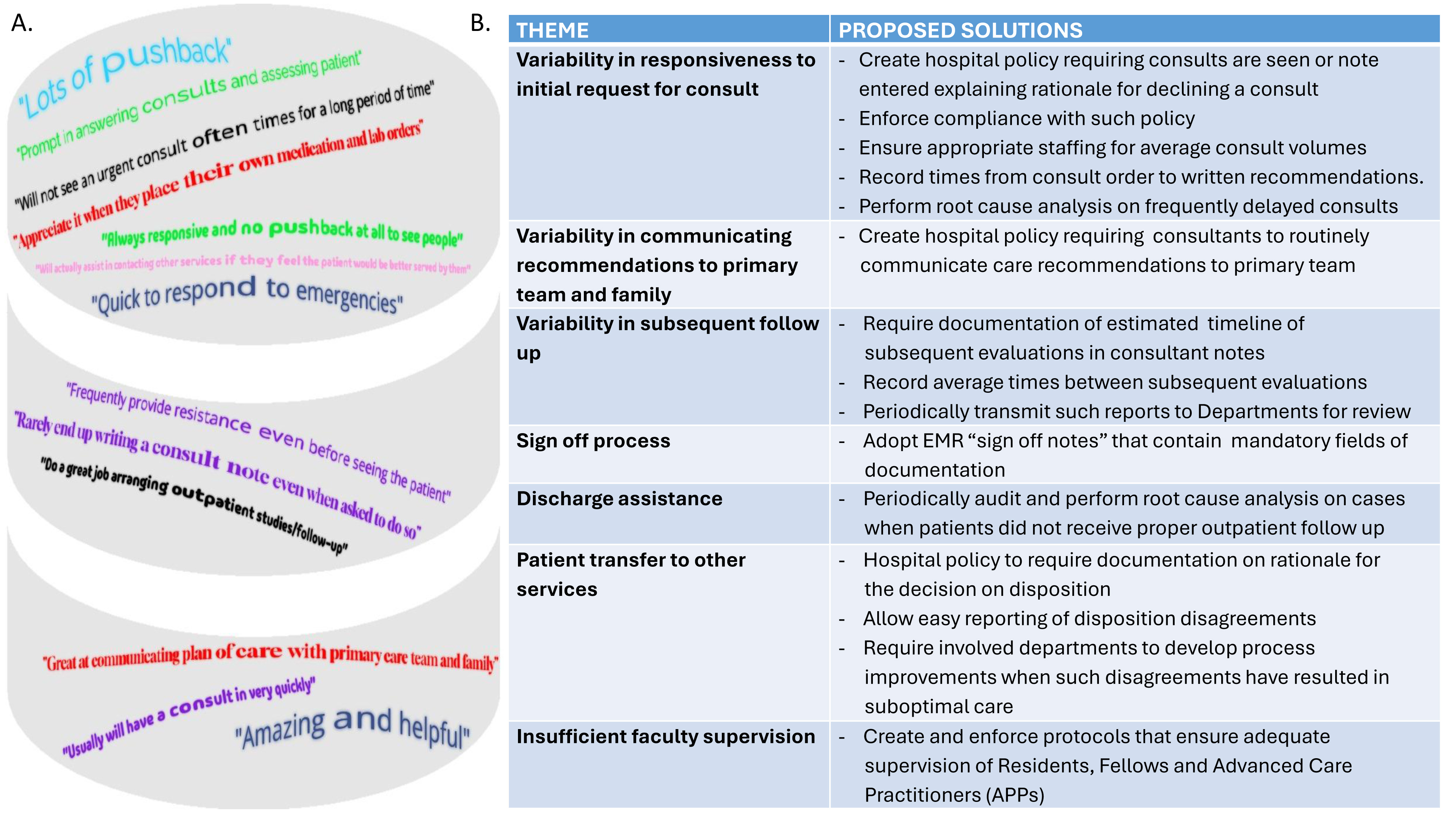
Results: A total of 510 comments from 239 responses were reviewed to generate 986 codes. Seven themes were generated and categorized into 2 domains: characteristics of consultant behavior and impact of consultant behaviors (Table 1). The most reported concerns were delays related to the initial consultation (mentioned 143 times) and issues related to agreeing to see the patient (85 times). Concerns about transitions of care were mentioned 47 times, while issues regarding quality of the recommendations and sign off process were both mentioned 46 times. Based on our results, we generated several recommendations to improve the consultation process (Fig. 1).
Conclusions: A qualitative analysis of comments made by frontline providers gave meaningful insight of the most common challenges in the consultation process at our Institution, and the themes generated allowed development of recommendations that could have a significant impact on hospitalist satisfaction with the consultation process and outcome metrics such as length of stay and readmission rates. Based on these results, we have created guidelines for consulting services at our institution that have been incorporated into our hospital bylaws3. Further research is needed to study consultant perceptions of hospitalist and ED consultation requests.