
Case Presentation:
A 65‐year‐old undomiciled man without known medical history presented to the hospital with fever amd right shoulder and knee pain. Following arthrocentesis, he was diagnosed with methicillin‐sensitive Staphylococcus aureus (MSSA) polyarthritis, thought to have originated from his urinary tract. Antibiotic therapy was initiated and surgical washout performed. He clinically improved until hospital day 5, when he was noted on rounds to be moaning, diaphoretic, and hypertensive to 217/108. On examination, he was noted to have abdominal distention, decreased bowel sounds, and a new right scrotal mass extending to his inguinal region. Palpation of the mass resulted in leakage of urine from the urethra. Computed tomography of the abdomen and pelvis (Figs. 1 and 2) revealed herniation of the majority of the urinary bladder and bilateral distal ureters along the inguinal canal and into the right scrotum, with associated severe hydroureter and hydronephrosis. General surgery was consulted and manually reduced the hernia with large amounts of voided urine. Urology placed a Foley catheter. His bladder continued to spontaneously herniate but remained amenable to manual reduction. Creatinine peaked at 3.5 mg/dL (admission baseline, 1.0 mg/dL) 4 days after this event. He later underwent unsuccessful surgical repair with mesh via the Stoppa procedure. His postoperative course was notable for a single episode of altered mental status requiring brief intubation, but he remained otherwise stable prior to his transfer to another facility. Creatinine had improved to 1.7 mg/dL on the day of discharge.

FIGURE 1. Computed tomography of the pelvis (horizontal section) demonstrating containment of the urinary bladder within the right hemiscrotum.
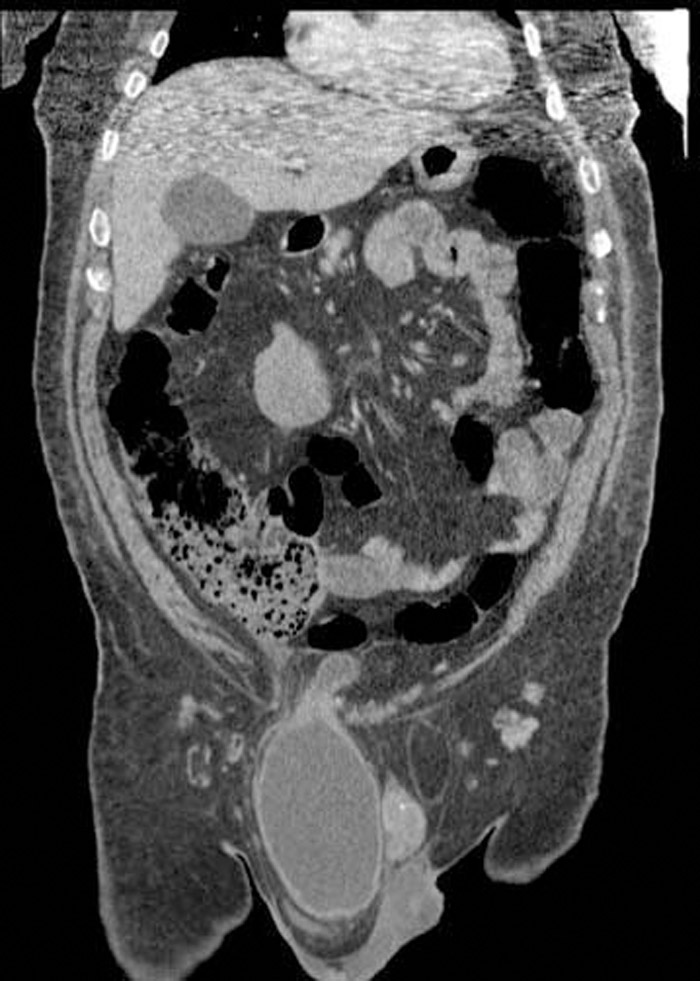
FIGURE 2. Computed tomography of the abdomen and pelvis (coronal section) again demonstrating near‐total herniation of bladder through the right inguinal canal into the right hemiscrotum. A small portion of the superior bladder remains intraperitoneal, resulting in an hourglass contour.
Discussion:
Although a small percentage of inguinal hernias involve the bladder, massive bladder herniation into the scrotum is extremely rare, with approximately 100 cases reported in the literature. Patients older than 50 years are at greatest risk and classically present with scrotal pain, inguinal or scrotal swelling and voiding disturbance. Right‐sided involvement is most common. Risk factors for bladder herniation include bladder outlet obstruction, diminished bladder tone, and sliding indirect or direct inguinal hernias. Obesity is often a contributor and may have been in this particular case. Whether a latent structural anomaly or hernia predisposed this patient to his initial MSSA urinary tract infection is unclear.
Conclusions:
We report a case of acute bladder herniation. Hospitalists should be familiar with this rare cause of acute abdominal or scrotal pain. Passage of urine in association with manipulation of the mass may suggest the diagnosis. Prompt imaging and reduction of the bladder is necessary in order to prevent renal complications and possible visceral strangulation. Urgent urologic and general surgical consultation is warranted.
Disclosures:
J. Best ‐ Oakstone Medical Publishing, CME reviewer