Background: Developing contextualized curricula in diagnostic reasoning and clinical decision-making is crucial to improve medical education (1,2). Barriers to transition from classroom-based to workplace curricula include workflow constraints, the absence of standardized tools to assess clinical reasoning, the complexity of decision making, and outdated teaching methods (3,5). Aimed to bridge these gaps, we developed the I-REASON (Improving REASONing) curriculum.
Purpose: – Improve trainee performance in hypothesis-driven data-gathering, problem representation, differential diagnosis prioritization, and appropriateness of testing/management as measured by the modified Assessment of Reasoning Tool (mART).- Improve trainee satisfaction with teaching and feedback on clinical reasoning and high-value decision making, measured by pre and post-intervention surveys.
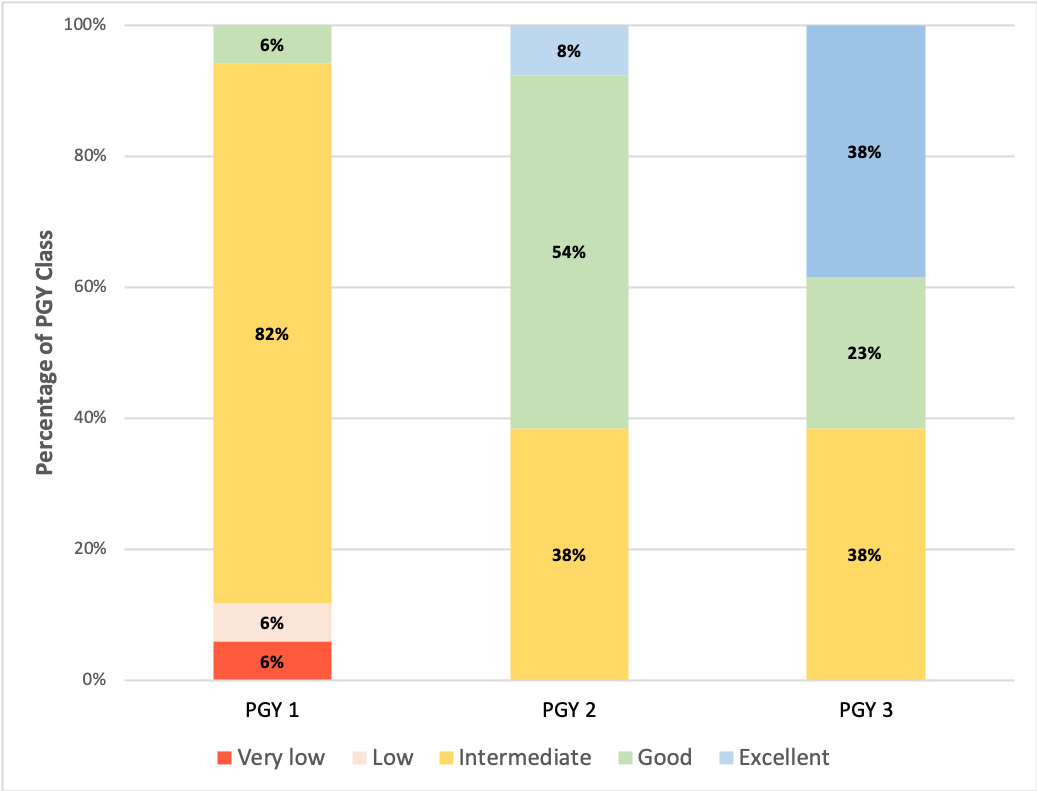
Description: I-REASON is being piloted at a community-based internal medicine residency program, affiliated to a tertiary care academic medical center. This project is part of a national collaboration supported by the Society to Improve Diagnosis in Medicine to develop curricula in diagnostic competencies. I- REASON includes three strategies:a) Implementing a cognitive tool to promote a deliberate approach to clinical reasoning: In addition to developing a solid clinical knowledge, mastering cognitive strategies is essential for effective problem-solving (6). Accordingly, we are implementing a framework (SOUND-REASOn) to guide problem representation, differential diagnosis prioritization, and high-value testing (Fig 1).b) Implementing a checklist for oral presentations: Building on prior initiatives to optimize the structure of oral presentations, such as SNAPPS (7–10), we are implementing a 6-point checklist based on the REASON framework to focus the oral presentations on critical elements of the diagnostic process and high-value decision-making. Attending physicians are expected to provide feedback on diagnostic strategies, point out diagnostic pitfalls, and emphasize on high-yield learning points. c) Implementing an assessment tool to enhance self-assessment, peer-to-peer, and faculty feedback on clinical reasoning. We are training faculty and residents in using a modified version of the assessment reasoning tool (mART) to provide a framework and a shared language to enhance self-direct learning, peer-to-peer, and faculty feedback (11). Notably, a set of high-quality instructional videos, created by the developers of the ART, are available to facilitate training.Preliminary results:- The pre-intervention assessment started in September 2019, and currently, it has involved 85% (17/20) of the first-year residents, 65% (13/20) of the second-year residents, and 65% (13/20) of the third-year residents. Half of the assessed residents scored intermediate, one-fourth scored good, and one-sixth scored excellent. As expected, scores improved along with the level of training (Table 1). Feedback from the proof of concept phase suggested that the acceptability of the program by faculty and residents was high.-The resident training sessions are planned for January of 2020, and the post-intervention assessment for March of 2020.
Conclusions: I-REASON is an innovative and promising practice-based curriculum that is piloting cognitive tools to enhance the teaching of clinical reasoning and high-value decision-making in the ward.