Case Presentation:
A 28‐year‐old Italian male with anorexia nervosa diagnosed 9 years ago, obsessive‐compulsive disorder (OCD), and hypogonadotropic hypogonadism, presented after he collapsed at work and was taken to a local emergency room for IV fluids and discharged home. He re‐presented a few days later with increasing fatigue. Over the prior three months, he had a worsening in his anorexia and OCD—caloric intake was less than 800 calories per day, he was running 10+ miles per day, and spending an additional 1.5 hours in the gym. There was a resultant 10‐pound weight loss in the prior two weeks. He denied B symptoms, recent travel, known exposures to radiation or chemicals. He has not been sexually active or had any sexually transmitted infections. Medications included testosterone IM, Vitamin D3, Multivitamin, Calcium, Fish oil, Whey protein powder. He denied herbal/supplement use, illicit drugs, or alcohol. His twin brother is healthy, but both his father and mother have psychiatric diseases (bipolar disorder and depression).
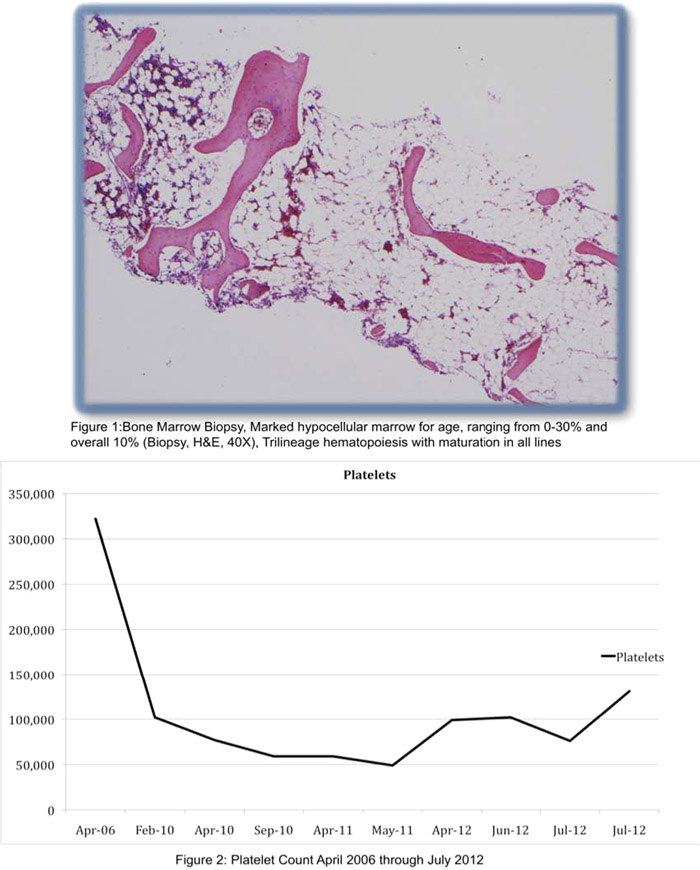
Physical examination revealed a cachectic malnourished appearing male (48kg) with dry mucus membranes, conjunctival pallor, no splenomegaly, no lymphadenopathy, and no petechiae. WBC count was 2200, hemoglobin 12.6, MCV 95.6, RDW 13.3, platelets 76,000, BMP and LFT WNL except low albumin, TSH 2.55, RPR NR, HIV negative, reticulocyte percent 1.35%. PNH Probe was negative. Chromosome analyses were normal (46XY). His platelet count was 77,000 in 2007 with the lowest count of 49,000 recorded in May 2011 (Figure 1).
Bone marrow biopsy revealed trilineage 10% hypocellular bone marrow (Figure 2).
Patient was admitted to the psychiatric ward and therapy was initiated. He continued with cognitive behavioral therapy as an outpatient, nutritional status improved, and OCD behaviors decreased. On follow‐up, his counts showed improvement with platelets of 131,000, the best they had been in 2 years.
Discussion:
Peripheral cell count abnormalities including all cell lines have been shown in AN. In four large retrospective studies, incidence of leucopenia ranged from 22‐36%, anemia 21‐39%, and thrombocytopenia 5‐11.3%(3‐8). Our patient had a platelet count nadir of 49,000, which is much lower than numbers cited in studies [184,000‐244,000] (4,8,10).
A large retrospective study looked at 80,000 bone marrows and found 155 cases of gelatinous bone marrow transformation (fat cell atrophy, focal loss hematopoietic cells, deposition of extracellular gelatinous substances). This was usually in adults (twice as likely in men than women), more severe in younger adults, and encompassed a variety of severe generalized illnesses—AN, febrile illnesses, AIDS, cancers (13).
There is a case report of a 12‐year‐old female with AN describing a complete serous atrophy of her bone marrow but interestingly, no peripheral cell count disturbances.(14) As can be seen from our patient, his peripheral counts were not as impressive as his 10% marrow hypocellularity.
Conclusions:
This is one of the few case reports of male anorexia leading to profound hypocellularity of the bone marrow. Interestingly, his peripheral counts were not as markedly low as would have been expected with such a hypocellular marrow. Bone marrow abnormalities (hypocellularity and gelatinous transformation) have been described in a select few case reports that show improvement in the bone marrow (and also in peripheral counts) occurring with adequate nutrition.