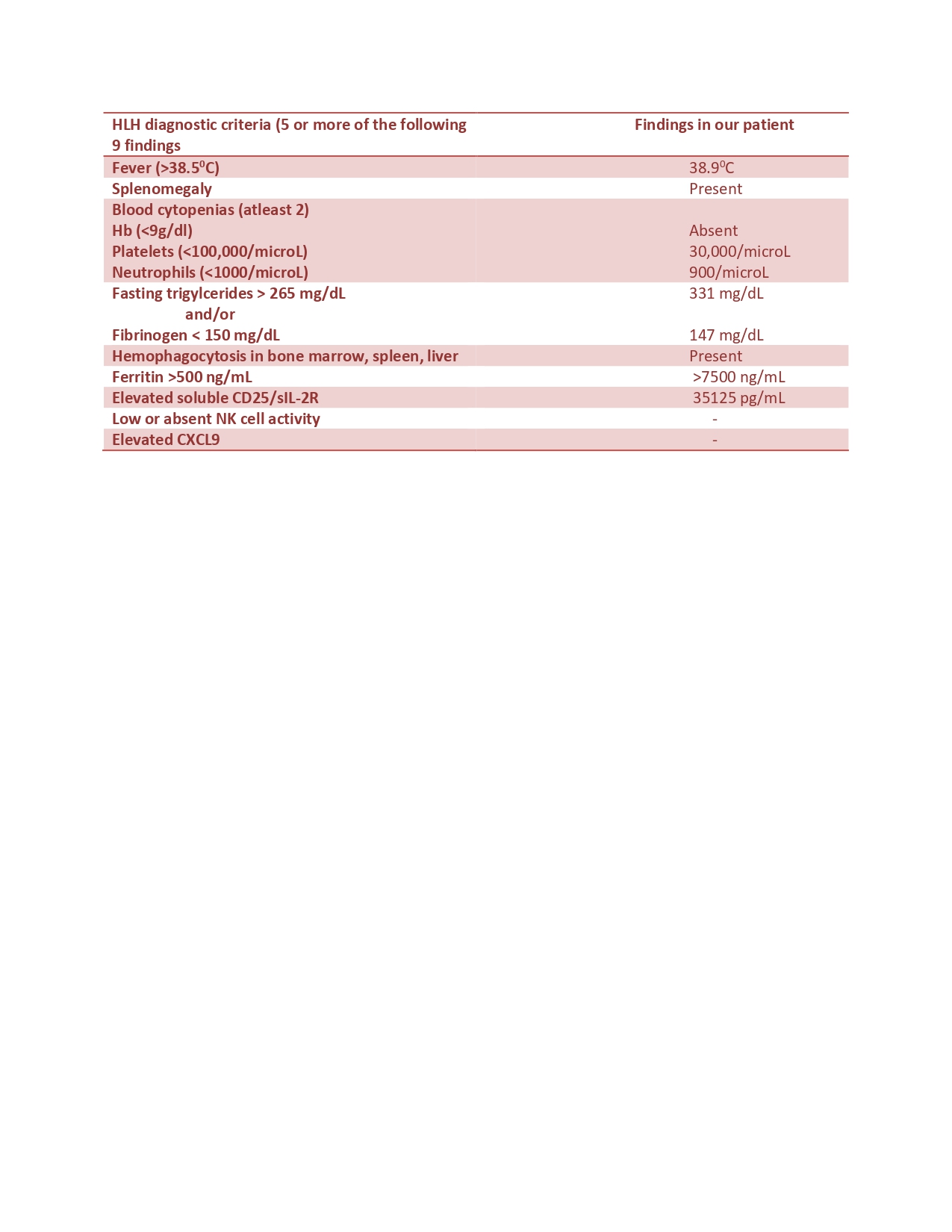
Case Presentation: A 27-year-old gentleman with no significant past medical history presented to our hospital with five days of persistent fevers with night sweats, sore throat, headache, vomiting, and neck pain. Upon initial evaluation, his temperature was 38.4° Celsius, heart rate of 130 beats/min, blood pressure of 126/78 mm of Hg, respiratory rate of 18 breaths/min, and he was saturating at 98% on room air. The physical examination was remarkable for mild splenomegaly. Laboratory findings were significant for a WBC count of 1800/microliter (reference range, 4500-11000), platelet count of 30,000/microliter (reference range, 150,000-450,000), AST of 474 Units/Liter (reference range, 8-33), ALT of 272 Units/Liter (reference range, 4-36), GGT of 135 Units/Liter (reference range 5-40), ALP of 187 Units/Liter (reference range, 44-147), total bilirubin of 2.2 mg/dl (reference range, 0.1-1.2), direct bilirubin of 0.5 mg/dl (reference range < 0.3), and LDH of 2995 Units/Liter (reference range, 105-333).Further workup including CT scans of the head, chest, abdomen, and pelvis; microbiologic cultures from blood, urine, and CSF; Urine and CSF analysis; viral serologies for HIV, HSV, CMV, VZV, HHV-6, and Hepatitis viruses, all were unremarkable. Ferritin levels obtained as part of the inflammatory workup were >7500 nanograms/milliliter (reference range, 12-300), and triglycerides at 331 mg/dl (reference range, < 150). EBV serologies were remarkable for EBV DNA Quantitative PCR of 51102 copies (4.71 log copies/ml).Hemophagocytic lymphohistiocytosis (HLH) secondary to EBV infection became the leading diagnosis now, and with worsening clinical status, the patient was empirically started on ganciclovir 5mg/kg IV BID. On day 3 of treatment, the patient started improving with defervescence of fevers and improvement in lab parameters. Bone marrow biopsy showed increased macrophages with hemophagocytosis. Soluble IL-2 receptor levels also returned elevated at 35125 picograms/milliliter (reference range, 532-1891), confirming the diagnosis of HLH with an H score of 228.
Discussion: HLH is a syndrome of multi organ failure caused by unchecked macrophage and lymphocyte mediated inflammation. Viral infections, especially EBV is a common trigger. Treatment is tailored based on the underlying cause such as antimicrobials for triggering infections, glucocorticoids for rheumatologic condition, or antineoplastics for cancers.EBV infection associated with HLH often occurs in immunosuppression or hematologic malignancies. Primary EBV infection or reactivation resulting in HLH in immunocompetent individuals remains distinctly uncommon. HLH has a high mortality rate, and there have been a few case reports describing the use of antivirals in EBV-associated HLH. They are underutilized and are usually used in conjunction with immunosuppressants. Our case highlights the successful treatment of EBV-associated HLH with antiviral monotherapy.
Conclusions: Our case is unique because of the remarkable recovery noted with ganciclovir. It also highlights the significance of having a high suspicion for EBV-associated HLH in the setting of persistent fevers, cytopenias, abnormal liver function tests, and markedly elevated ferritin and triglycerides. Further research is required to assess the response of different antivirals in infection-triggered HLH and to study the natural history of the infection and spontaneous clearance in clinically stable HLH patients.