Background: Involvement of a cardiologist in the care of hospitalized patients with a primary diagnosis of heart failure (HF) has been shown to improve outcomes and may affect their readmission rates. However, less is known about the patients admitted for a different reason who carry a secondary diagnosis of HF and the effect of cardiology consultation on their outcomes. We hypothesized that involvement of a cardiologist for patients admitted with a secondary diagnosis of HF on a general medicine service reduces readmissions at 0-30 days or 31-90 days.
Methods: The study was based on admissions from a 600-bed academic, urban, tertiary, referral hospital from January 2012 to May 2017. Patients with a discharge diagnosis of HF not specified as primary who were admitted to a general medicine service were included. Demographics, medical history, and clinical data on admission were obtained. Presence of cardiologist consultation during admission was determined by identification of cardiology consult notes in the medical record. The primary outcome was any hospital encounter dated within the subsequent 90 days from discharge. Patients who died during the index hospitalization were excluded from the analysis. Unadjusted and multivariate adjusted analyses were completed for the primary outcome to compare readmissions between patients with or without cardiologist consultation.
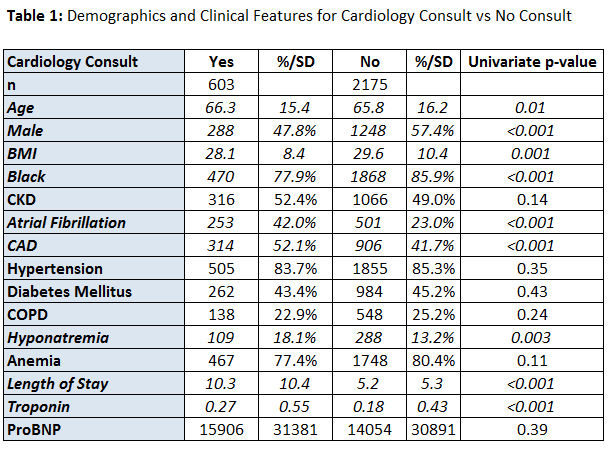
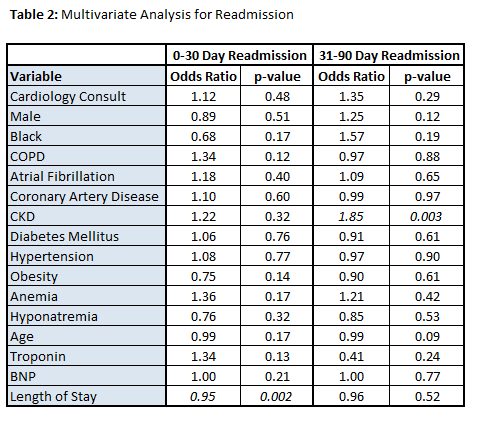
Results: A total of 2778 patients were admitted with a secondary discharge of HF during the study period with 603 (21.7%) receiving a cardiology consultation. Patient receiving cardiology consultations were more likely to be older, male, Black, and suffer from more chronic cardiac conditions. A complete summary of demographic is compiled in Table 1. The rates of readmission were similar between both groups at 0-30 days and 30-90 days in the unadjusted analysis. In a multivariate model, readmission was driven by multiple demographic factors, but cardiology consultation did not have a significant effect (Table 2).
Conclusions: Cardiology consultation was not associated with a difference in readmission rates at 30 and 90 days in unadjusted and multivariate analyses in patients admitted to a general medicine service with a secondary discharge diagnosis of HF. Readmission risk is associated with a variety of factors, including social one, which could not be affected by consultation alone, therefore the impact of consultation on this population may require further investigation.