Background:
Patients admitted to our hospital with possible Acute Coronary Syndrome (ACS) have a length of stay exceeding the community average. We postulated that the admitting residents were deferring the decision to order a stress test to the attending of record or cardiology consult. We hypothesized that implementation of a clinical decision support tool (CDST) would increase the appropriate and timely ordering of cardiac stress tests.
Methods:
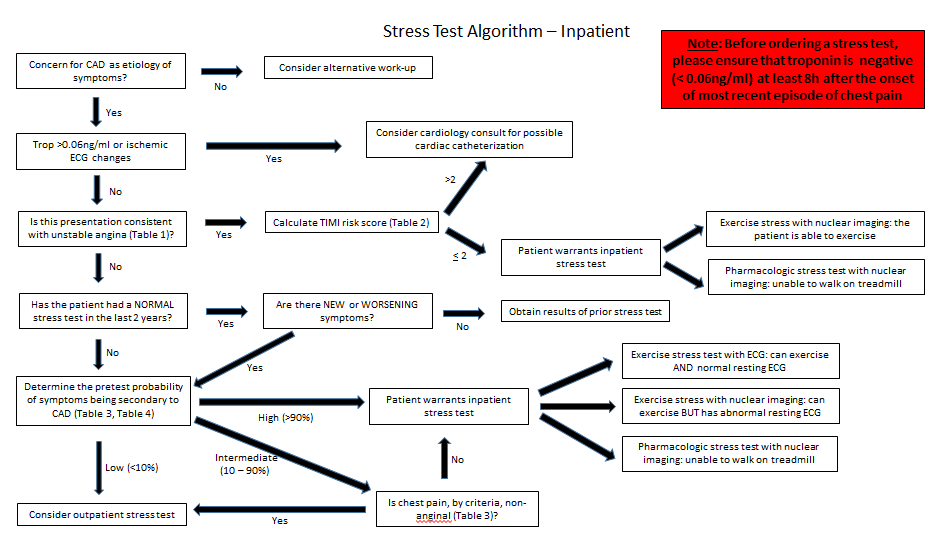
A CDST was created in collaboration with the cardiology service and subsequently dispersed to the admitting housestaff starting July 1, 2015 (Figure 1). Feedback was solicited during the initial implementation phase though no modification to the CDST was made.
We compared the cohort of patients admitted with appropriate cardiac diagnoses during the four months prior to the implementation of the CDST (March through June 2015) with patients admitted during the four months after implementation (July through October 2015). The primary outcomes were average length of stay (ALOS), rate of stress test performed, and the rate of positive stress test. Housestaff were surveyed about their reactions to the CDST.
Results:
Prior to the intervention 717 patients were admitted with chest pain, whereas 602 patients were admitted with chest pain after the intervention. The rate of stress tests went from 28.6% prior to the intervention to 21.1% after the intervention (p < 0.01). The difference in rates of abnormal stress tests and ALOS were not statistically significant.
The survey response rate was 54% for the admitting residents (25/46). When asked if they use the CDST for guidance when they have difficulty deciding whether or not to order a stress test, 36% said “never” whereas 28% said either “often” or “always”. A majority (58.3%) of residents agreed or strongly agreed that the decision support tool is a helpful resource, and 54.2% of residents agreed or strongly agreed that they would recommend the tool to others.
Conclusions:
The implementation of a CDST was associated with a significant decrease in the rate of inpatient stress tests performed at our hospital. The rate of abnormal stress tests was unchanged, suggesting that the CDST may have led to the ordering of fewer tests that likely would ultimately have been negative. The survey data suggests that the majority of residents find the tool helpful, however there is still a cohort of residents who never use CDST. Increasing resident use of the CDST has potential to decrease unnecessary testing and reduce ALOS, and may be achieved through integration of the CDST into workflow, for example by embedding it in the electronic ordering system.