Background: Pulmonary embolism (PE) is the third most common cause of death from cardiovascular disease despite significant improvements in diagnosis and management in recent years. PE patients are risk-stratified to guide treatment, and multidisciplinary PE response teams (PERTs) have been established to optimize patient care. This study aims to compare PE patient outcomes over a 12-month period both before and after implementation of a PERT at a large academic hospital.
Methods: The PERT was established in October of 2023 as a collaborative effort amongst faculty from pulmonary hypertension (PH), critical care, interventional radiology, and cardiovascular thoracic surgery. Physicians throughout the hospital were trained to risk stratify PE patients at the time of diagnosis and all intermediate-high risk and high-risk patients were to be discussed with the PERT leader to determine whether PERT activation was appropriate. A PERT activation provided immediate access to a team of experts to guide care. Additionally, emergency room physicians were asked to admit all patients with a primary diagnosis of PE to the PH service, unless the patient’s comorbidities necessitated admission to a different service. Physicians throughout the hospital were also educated on evidence-based practices for PE patients, including anticoagulant choice. The charts of all patients with a primary diagnosis of acute PE during the pre-PERT (10/22-9/23) and post-PERT (10/23-9/24) periods were reviewed to determine risk stratification, PH admission and consultation rates, PERT consultation rate, anticoagulation use, length of stay (LOS), and mortality rate.
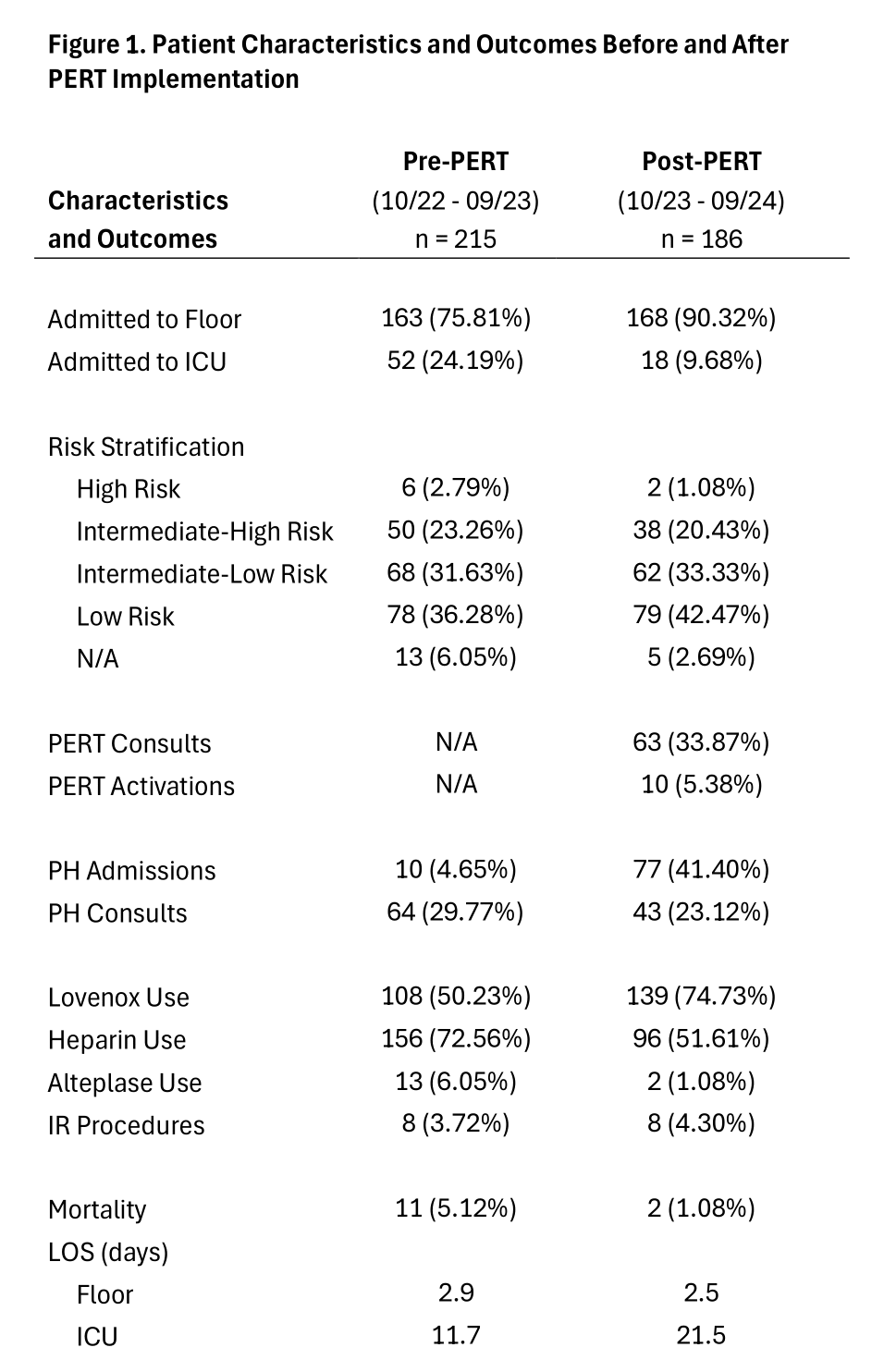
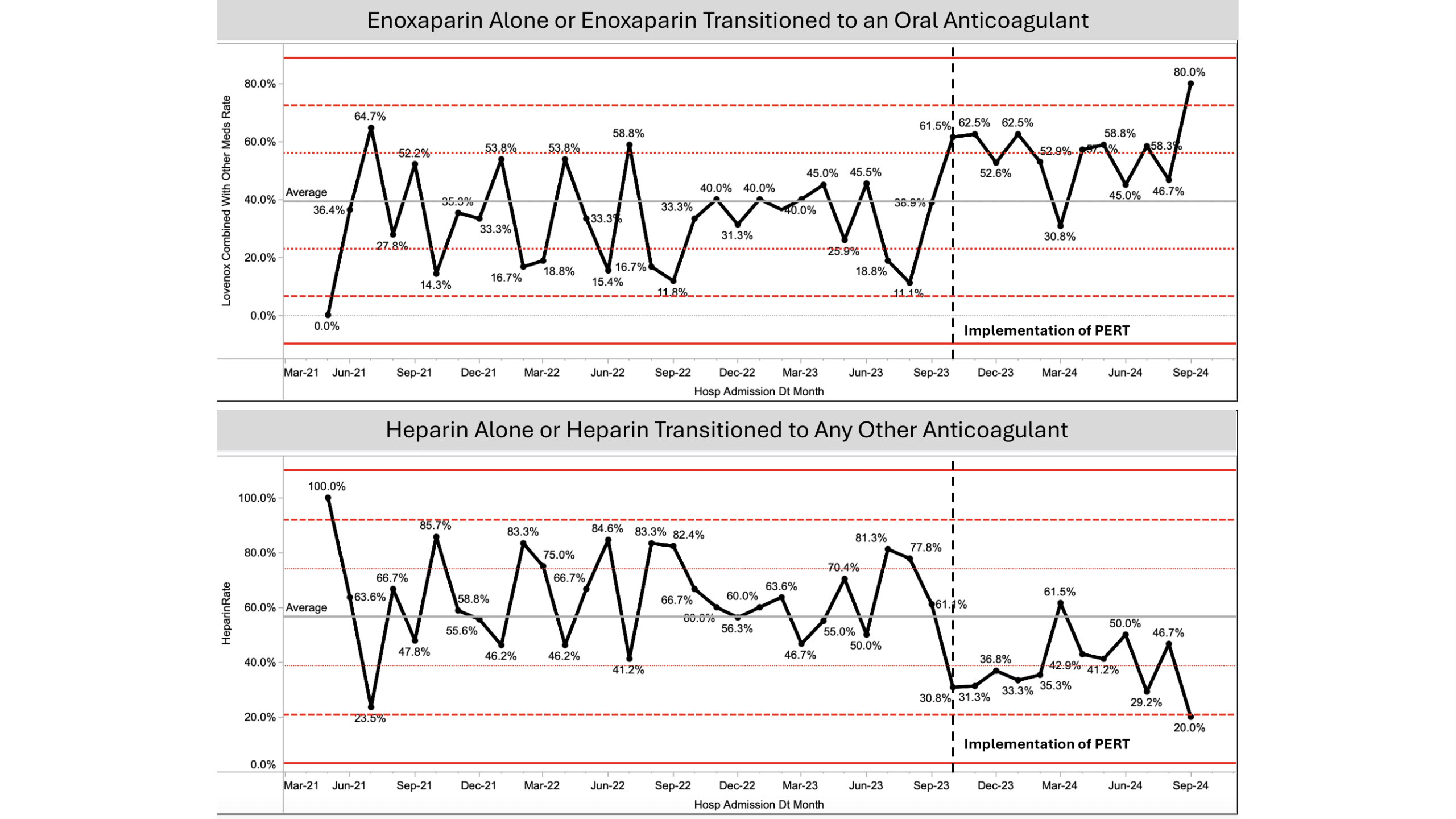
Results: Of 215 patients with acute PE in the pre-PERT period, 52 were admitted to the intensive care unit (ICU), and 163 were admitted to the floor (24.19% vs. 75.81%). Risk stratification was as follows: 6 patients (2.79%) were high risk, 50 (23.26%) were intermediate-high risk, 68 (31.63%) were intermediate-low risk, 78 (36.28%) were low risk, and 13 (6.05%) did not have enough data. 10 patients (4.65%) were admitted to the PH service, and 64 (29.77%) received PH consults. Enoxaparin was used in 108 patients (50.23%) and heparin was used in 156 patients (72.56%). Floor LOS was 2.9 days and 11 patients (5.12%) died during hospitalization.In the post-PERT period, of 186 patients with acute PE, 18 were admitted to the ICU and 168 were admitted to the floor (9.68% vs. 90.32%). Risk stratification was as follows: 2 patients (1.08%) were high risk, 38 (20.43%) were intermediate-high risk, 62 (33.33%) were intermediate-low risk, 79 (42.47%) were low risk, and 5 (2.69%) did not have enough data. 63 patients (33.87%) were discussed with the PERT leader and 10 (5.38%) received a PERT activation. 77 patients (41.40%) were admitted to the PH service, and 43 (23.12%) received PH consults. Enoxaparin was used in 139 patients (74.73%) and heparin was used in 95 patients (51.61%). Floor LOS was 2.5 days. 2 patients (1.08%) died during hospitalization, which is significantly decreased from the pre-PERT period (p = 0.0244).
Conclusions: After PERT implementation, enoxaparin usage increased while heparin usage decreased. Additionally, mortality and floor LOS both decreased. The implementation of the PERT, hospital wide education on best practice, and an increase in specialized care for PE patients led to improved patient outcomes. Further study is needed to determine if this mortality trend continues, as the pre-PERT cohort was comprised of a higher number of patients admitted to the ICU and deemed high risk.