Background: Chronic hepatitis C virus (HCV) is a leading cause of liver failure and cancer. Half of 3.5 million infected persons in the U.S. know their status, and 43% have access to care. Despite antivirals that make HCV curable, barriers persist including insufficient screening and late diagnosis. Many infected individuals access healthcare but are not tested until symptomatic.
In Baltimore, HCV is suspected to be underdiagnosed and undertreated. Recent data suggest 7% prevalence as compared to 1% nationally, and that 25% of patients would not be screened using current criteria.
Purpose: Hospitals can address missed opportunities for HCV diagnosis and linkage to care. A program was implemented to routinely offer HCV testing to patients admitted to the Departments of Medicine and Family Medicine (DOM/FM). Without testing confirmation of chronic HCV, patients cannot be linked to care. Through universal screening, the aim was to increase the proportion of patients tested and connected to care. Further, patients with known HCV admitted to DOM/FM and four surgical services were offered linkage to outpatient care.
Description: A multidisciplinary, routine HIV testing program provided the infrastructure to integrate routine HCV testing. Streamlining the two programs was balanced with customization for differences in HIV/HCV testing guidelines. Limited national routine HCV testing experience required innovative protocol development. Without consensus on repeat testing, policies were developed for identifying ongoing risk and appropriate screening intervals. Additionally, the potential to achieve cure presented new process considerations for people at risk for reinfection.
Recognizing the potentially high number of patients needing care, a clear linkage process was vital. Referral algorithms were created based on HIV co-infection and care needs and established milestones for follow-up. Processes were devised to track patients lost to follow-up and aid concurrent efforts to build city surveillance.
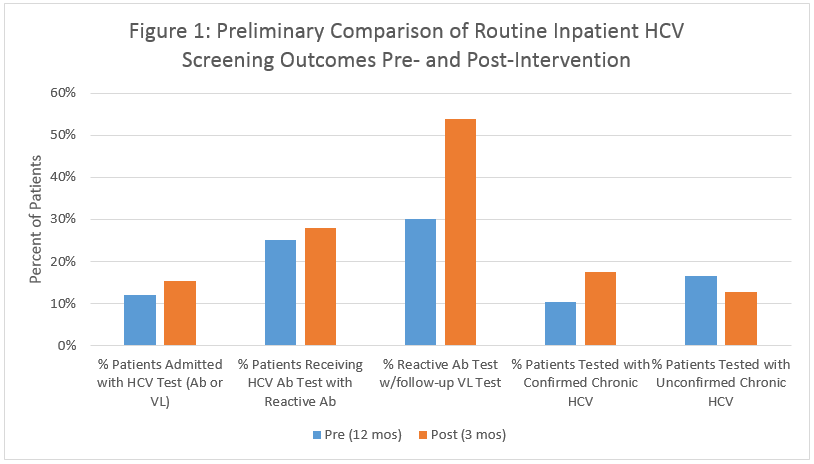
Physicians and nurses were educated on the integrated protocol. Daily/monthly reports are reviewed to reinforce program goals and ensure continuous quality improvement. Screening rates were compared to the prior 12 months. In the first 3 months post-intervention, 160 (15%) patients were screened. Screening continues to increase and confirmation testing has improved. Of those with a reactive antibody test, 54% received viral load confirmation compared to 30% pre-intervention. HCV rates are high at 18% chronic HCV and 13% unconfirmed chronic HCV. Of 87 previously positive patients encountered, 68% were out of care.
Conclusions: By removing barriers to identifying infection, access to HCV care will improve, ultimately decreasing HCV morbidity and mortality in Baltimore.