Background: Managing clinical deterioration in hospitalized patients is a major component of patient care. When medical students transition to residency, they are expected to manage patients who acutely decompensate in rapid response scenarios, often without dedicated training or exposure on their clerkship rotations. Simulation center training (SIM) has been utilized to help trainees recognize and respond to deteriorating patients and build confidence in handling these scenarios. It has rarely been part of the sub-internship clerkship.
Purpose: To incorporate a structured Rapid Response SIM into the Direct Care Hospitalist Service (DCHS) sub-internship rotation.
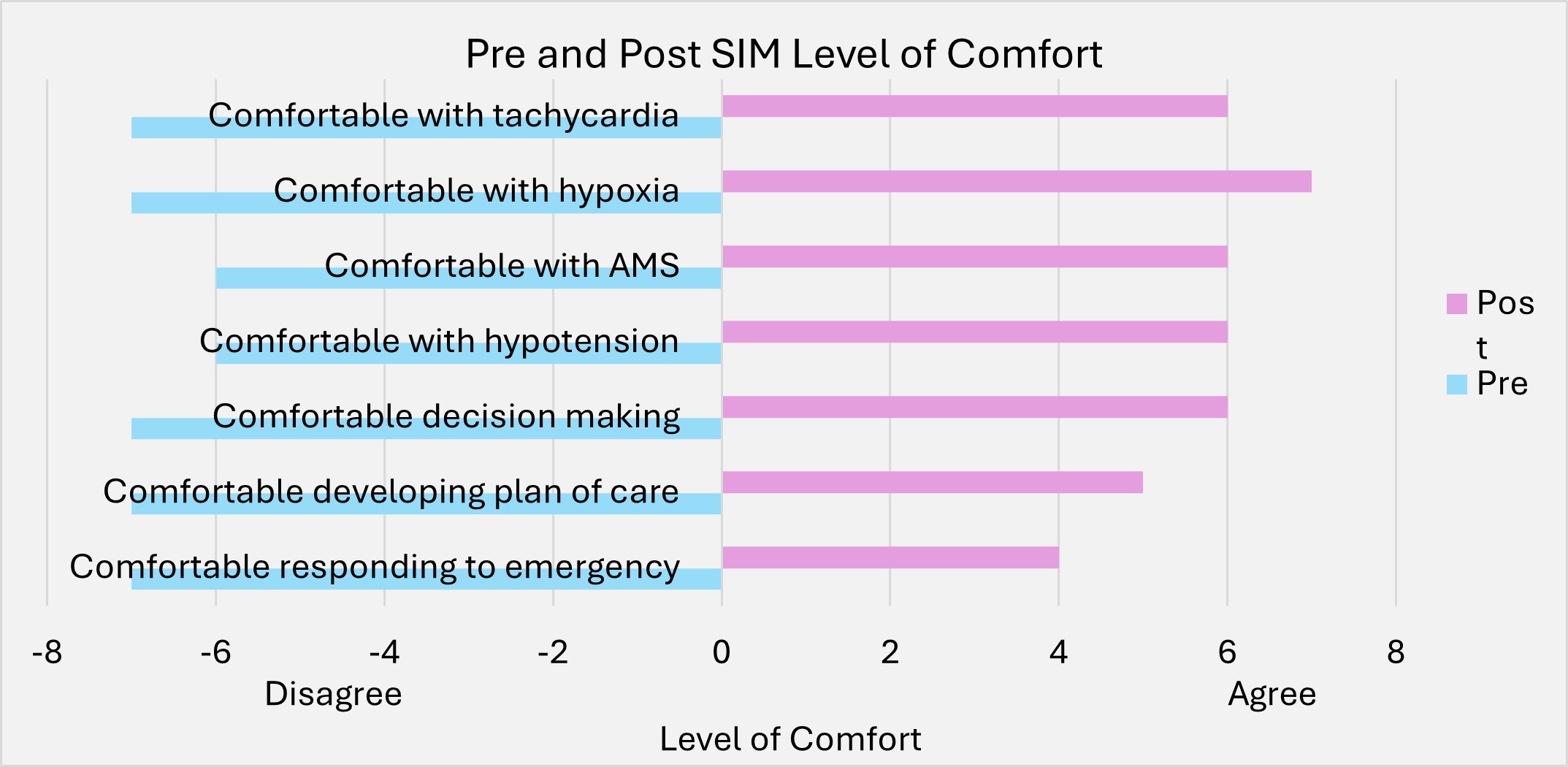
Description: A 2-hour SIM was incorporated into the DCHS sub-internship made up of four cases of common decompensation scenarios including hypotension, tachyarrhythmias, respiratory distress, and altered mental status. The SIM was conducted after the students completed their 3 weeks of day service prior to transition to night shifts which included cross-cover of up to 22 patients. Prior to SIM, a survey was distributed assessing the students’ understanding of common rapid responses scenarios, triaging patients based on clinical instability, and their level of comfort when responding to various emergencies. Students alternate leading the team responding to medical emergencies. Following the session, the students completed 5 supervised night shifts. After completing their night shifts, the students were re-sent the initial survey with the inclusion of an open response section. 8 students participated in our SIM training. Prior to SIM, 4/8 (50%) of the students had never participated in a rapid response with the other 50% having participated in 1-2 rapid responses. 7/8 (87.5%) of students were correctly able to identify the most common cause of rapid responses hospitalized patients but only 2/8 (12.5%) were able to correctly identify the members of a rapid response team. 7/8 (87.5%) of students were uncomfortable responding to in-hospital emergencies, developing a plan of care for decompensating patients, managing hypotension, or managing hypoxia. None of our students felt comfortable managing patients with altered mental status or acute onset tachycardia. Following training, 100% of our students were able to identify the most common cause of rapid responses and identify the members of a rapid response team. 5/8 (62.5%) of students were comfortable responding to in-hospital emergencies. 6/8 (75%) were comfortable developing a plan of care for decompensating patients. 5/8 (62.5%) in managing hypotension, 6/8 (75%) managing altered mentation and tachycardia, and 7/8 (87.5%) managing hypoxia.
Conclusions: There was a vast improvement in student level of comfort managing patients with hypoxia, tachycardia, hypotension, and altered mentation. Though most students indicated that the simulation training enabled their preparedness to lead RRTs, we do not know how well this experience translates to the clinical setting. We aim to collect data 6- months into their intern year to explore residents’ reflections on real-life experiences as well as whether the simulation impacted their preparedness to lead real-life RRTs.