Background: Up to 12% of hospitalized patients require high dose parenteral thiamine treatment to prevent Wernicke’s Encephalopathy, a devastating and easily preventable neurologic disorder that can lead to death. Despite the fact that it is as simple and relatively inexpensive therapy with no known side effects, high dose thiamine continues to be underutilized. Attempts to improve thiamine use have had limited success. To more reliably prescribe high dose parenteral thiamine in our hospital, we implemented changes to our computerized physician order entry system with the goal of preventing Wernicke’s Encephalopathy in our patients.
Methods: This is a pre-post evaluation of a Quality Improvement project designed to increase the delivery of evidence-based high-dose parenteral thiamine to adult admitted patients at risk for Wernicke’s Encephalopathy at a large, urban, academic medical center. The intervention consisted of targeted EMR-based decision support at the level of the thiamine order, encouraging providers to order high-dose parenteral thiamine ( ≥200mg intravenous or intramuscular) ) dosed for patients with alcohol use disorder. The outcome measure was an order for high-dose parenteral thiamine defined as ≥ 200mg IV or IM. All admissions with an ICD code for alcohol-related diagnosis were examined in the year prior and year following the intervention. We examined time to first order of high dose parenteral thiamine using the method of Kaplan and Meier and compared the proportion of admissions with high dose order within 24 hours of admission time using univariate and multivariate logistic regression models. In addition, Control Chart methodology was utilized to detect special cause variation during the 2-year study period.
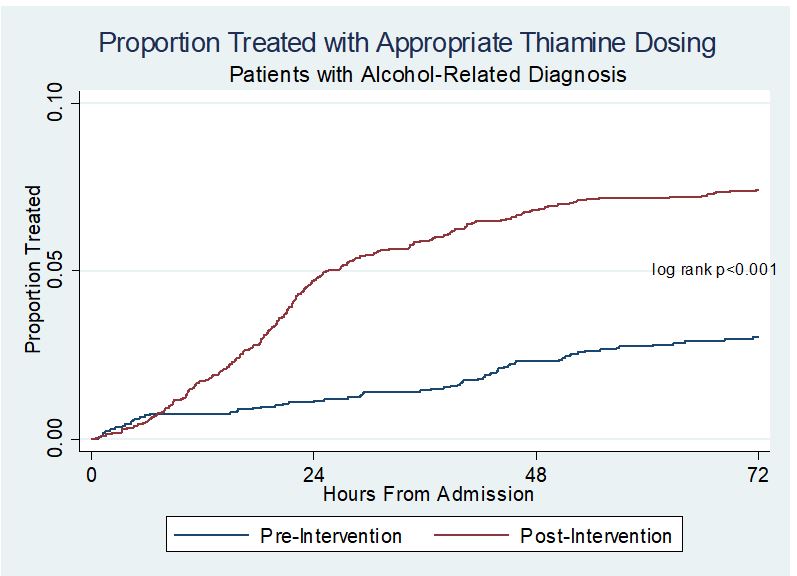
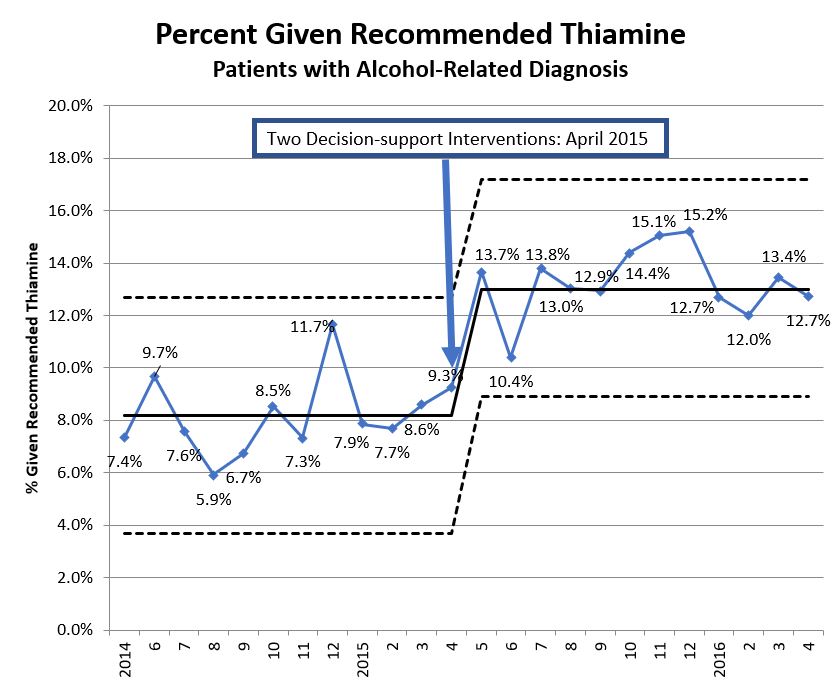
Results: There were 2,285 admissions with an alcohol-related diagnosis in the pre-period and 3,022 in the post-period. Time to high dose parenteral thiamine was significantly improved among post-intervention admissions compared with pre-intervention admissions (log-rank p<0.001, Figure 1). The post intervention period was associated with increased odds of a high dose thiamine order within 24 hours of admission in unadjusted (ORunadj 4.28, 95% CI: 2.81-6.53) and adjusted analyses (ORadj 4.50, 95% CI: 2.94-6.87). A control chart demonstrated special cause improvement in the first month after the intervention, with a sustained change in centerline from 8% to 13% of admissions that received high dose parenteral thiamine during the admission.
Conclusions: A simple EMR-based decision support tool can result in a sustained significant improvement in evidence-based high-dose parenteral thiamine prescribing in patients with alcohol-related diagnoses.