Background: The 12-lead electrocardiogram (ECG) is an essential tool when evaluating patients with suspected cardiopulmonary disease and inaccurate ECG interpretation may result in adverse patient outcomes. The Alliance for Academic Internal Medicine stated that ECG interpretation should be a skill required for medical school transition to residency. Yet, prior research indicates graduating medical students correctly identify an average of 8.2 of 22 common ECG findings and only 3.4 of 6 life-threatening diagnoses.The spacing effect is one of the most evidenced based components of adult learning theory. Evidence shows long-term retention is maximized by repeated exposure to the material over spaced intervals; however, this is underutilized in medical education. We implemented a spaced repetition ECG curriculum using online quizzes combined with group learning didactics. We hypothesized that a spaced learning curriculum would improve ECG interpretation skills on a posttest compared to students who received the group didactics alone.
Methods: The study included 140 students from the University of Colorado School of Medicine (CUSOM) entering their clinical clerkships. The CUSOM includes eight sites with both traditional block clerkships (TBC) and Longitudinal Integrated Clerkships (LIC).The control ECG curriculum (block control) for the TBC students included six group learning didactic sessions delivered during the 8-week clerkship. Students attended a 2-hour introduction to ECG interpretation lecture, followed by five 30-minute didactic sessions. A second control group included students enrolled in the LIC (LIC control). Students attended the same didactic series; however, the sessions were spaced over the course of the clinical year rather than 8 weeks. The intervention group included LIC students (LIC intervention) who attended the same didactic series spread over the course of the year; however, these students participated in the additional online spaced repetition quizzes. Online quizzes provided immediate feedback with answer keys illustrating key features with annotated ECGs. Students completed 16-18 ECG quizzes over the year spaced every 2-3 weeks apart. All students completed an extended multiple choice 17-item posttest at the end of their clinical year.
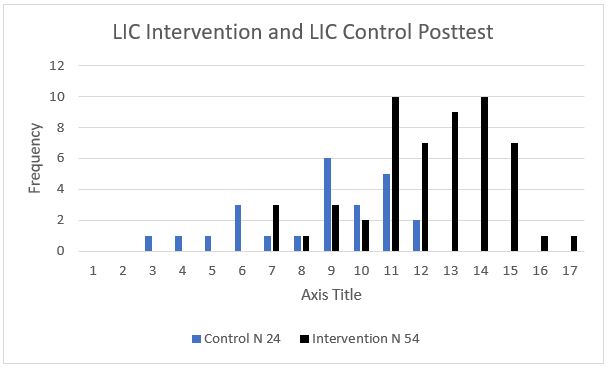
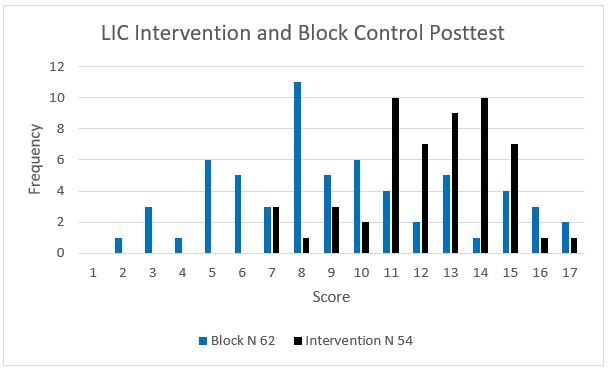
Results: The block control group contained 62 students, 24 in the LIC control group, and 54 were in the LIC intervention group. The ANOVA test was significant (F = 17.1, p < 0.001). Games-Howell post-hoc tests and were conducted and Hedge’s g was calculated to determine the effect size of the intervention. The mean posttest score in the LIC intervention group was significantly higher compared to the LIC control group with significant effect size (mean 12.4 vs. 8.6, Hedge’s g = 1.57, p < 0.001) and significantly higher in the LIC intervention group compared to the block control group (mean 12.4 vs. 9.4, Hedge’s g = 0.86, p < 0.001). There was no significant difference between the LIC control and block control groups (p = 0.59). Figures 1 and 2 provide a cluster chart comparing scores between the three groups.
Conclusions: An ECG curriculum incorporating intentional spaced repetition testing using quizzes that provide immediate feedback on a systematic approach to ECG interpretation improved ECG interpretation skills on an ECG posttest. These brief quizzes mitigate the impact of the forgetting curve and maintain student competency in ECG interpretation.