Background:
Accurate and timely documentation is essential for patient care, as well as the appropriate reflection of patient complexity and severity of illness. Most hospitals utilize a traditional retrospective or contemporaneous physician-query strategy to ensure documentation accurately impacts performance data, reputation/ranking, and reimbursement.
Purpose:
Here, we highlight three unique, hospitalist-driven interventions to support accurate documentation and clinical practice that – along with the development and maturation of a core clinical documentation improvement (CDI) program – have markedly impacted our institution’s risk-adjusted patient outcomes.
Description:
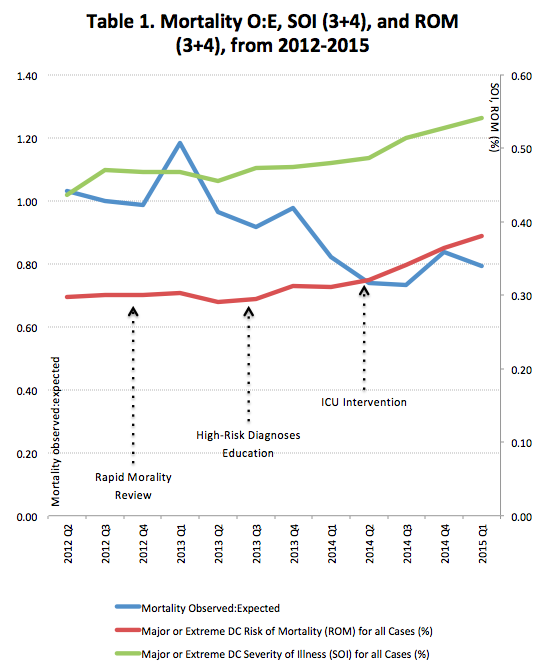
Rapid Mortality Review (RMR): with the support of a core group of hospitalist faculty, all mortalities on general medicine, hospitalist, geriatric, oncology, and ICU services are reviewed within 24-48 hours of a patient’s death. The aim of RMR is two-fold: (1) to understand the clinical care and what may have led to the patient’s death, and (2) to ensure that all relevant health conditions are documented and reflect the patient’s severity of illness and risk of mortality. Through systematic review of our deceased patients, we identified a number of CDI areas of improvement, including: identification of high risk conditions; specification of high-risk conditions; identification of patients who were DNR, receiving hospice care, and/or receiving end-of-life care measures.
MD Education and Identification of High-Risk Diagnoses: for inpatients, the identification of a small subset of high- risk conditions – sepsis, acute and chronic organ failure, malnutrition, and diabetes – have a major impact on a number of important patient outcomes including risk-adjustment mortality, length of stay and severity-indexed payment (MS-DRG). In this ongoing intervention, we emphasize the recognition and documentation of high-risk diagnoses for inpatients (on both medical and surgical services). For this effort, we created educational, on-the-fly references, and adapted the templating library in our EMR to assist physicians with accurately documenting these conditions.
Targeted CDI for the Highest Risk patients: we reviewed a random selection of ICU patient over a two month period and compared the specificity of documentation for three conditions (sepsis, respiratory failure, and heart failure) in the year prior to and following a brief educational initiative, focused on our housestaff rotating thru the medical ICU. Compared to the year prior, the odds of having “specific diagnoses” following our intervention was 2.3 the base (95% CI 1.23-4.29, p = 0.009), even controlling for discharge disposition, ICU length of stay, and total hospital length of stay.
Conclusions:
In addition to traditional approaches, targeted hospitalist-driven CDI interventions can improve the accuracy of inpatient documentation and may have a marked impact on the risk-adjusted outcome measures (see Table 1).