
Background: Syphilis cases in the United States increased by 42% from 2020 to 2024. In San Francisco, between 2019 and 2023, syphilis diagnoses increased by 18% among women, and congenital syphilis cases increased by 425%. The San Francisco Department of Public Health (SFDPH) recommends annual syphilis screening for all sexually active individuals between 15 and 44 years of age, and more frequent screening depending on risk factors. Hospital admissions provide a unique opportunity to screen at-risk patients. While approximately 40% of patients admitted to Internal Medicine services at an urban, safety-net teaching hospital meet SFDPH criteria for syphilis screening, over 70% were not screened.
Methods: We implemented an incentive-based quality improvement (QI) project to increase syphilis screening in at-risk patients admitted to Internal Medicine services. The project was advanced iteratively using A3 methodology. The initial intervention (August 2022) included educational resources and monthly feedback around screening rates, an updated admission order set included opt-in syphilis testing for at-risk patients (January 2023), and a final update involved opt-out testing within the admission order set (February 2024). We extracted data on syphilis screening for all at-risk patients admitted from January 2021 through June 2025. We calculated the screening rate before the intervention and after each improvement cycle. We used a logistic regression model to estimate the association between each intervention and syphilis screening, adjusting for demographics and risk factors. Individual risk factors were also assessed as potential effect modifiers. Changes in the rate of abnormal syphilis tests were analyzed as a proxy for new diagnoses.
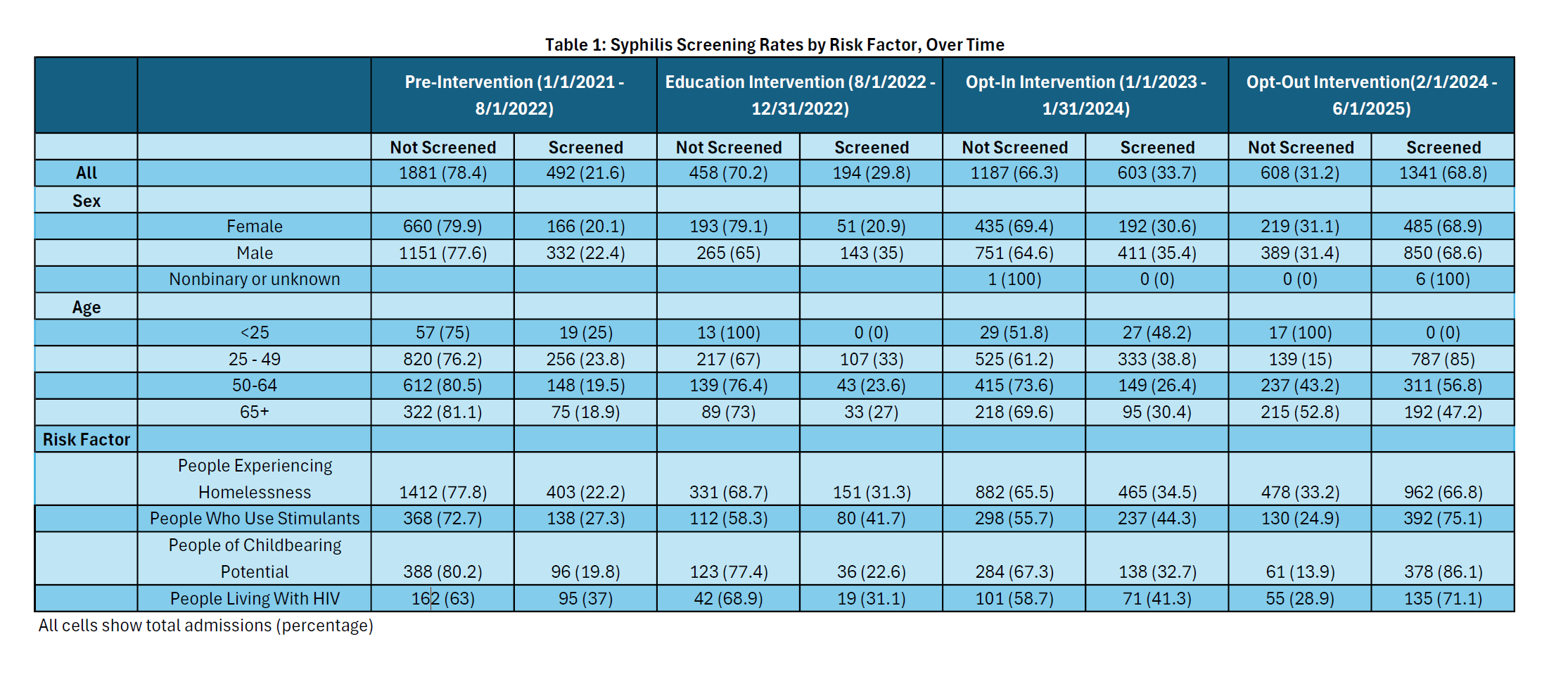
Results: There were 6,764 unique admissions of at-risk patients during the study period. At baseline, 21.6% of these patients were screened for syphilis. The screening rate increased after each intervention, reaching 68.8% with opt-out screening in effect. Although every at-risk group experienced increased syphilis screening rates, there was variation across risk factors. The largest improvement was observed among people of childbearing potential, with screening rates increasing from 19.8% to 86.1%. When taking into account multiple hypothesis testing, only the opt-out intervention was associated with increased syphilis screening with odds ratio (OR) of 3.7 (p < 0.0001). People of childbearing potential had an additional effect beyond that observed for all at-risk groups, with the interaction between opt-out intervention and this group having an OR of 6.0 (p < 0.0001). While the percentage of syphilis tests that were abnormal (positive TPA or elevated RPR) decreased, consistent with a shift from symptomatic testing to screening, the percentage of admissions of at-risk patients with abnormal syphilis tests increased for all groups over the duration of the study.
Conclusions: The addition of opt-out syphilis testing led to an increase in syphilis screening for at-risk patients admitted to an urban safety-net hospital. The effect was largest for people of childbearing potential, an especially important group given ongoing increases in syphilis infection rates among women and rising rates of congenital syphilis in San Francisco. While this screening initiative led to increased rates of abnormal syphilis test results, further study is needed to determine whether this intervention resulted in new syphilis diagnoses and linkage to treatment.
.png)