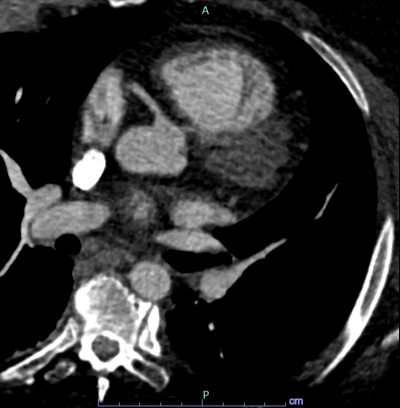
Case Presentation: A 36 year old female with a past medical history of hypothyroidism, type two diabetes, asthma, polycystic ovarian syndrome, and bipolar disorder presents with sharp chest pain that radiates to her left neck and arm. She states that the pain started suddenly when she was sitting 10 hours ago and gets worse with exertion. She had one episode of similar chest pain in the past since 2012 and had an unremarkable stress test. In the emergency department, her vitals were within normal range. Physical examination revealed some tenderness to palpation of her left upper quadrant. She had an observed episode of syncope upon standing, lasting a few seconds. Pertinent laboratory findings included LFTs within normal limits, negative D-dimer, and three negative troponins. EKG showed T-wave inversion in the precordial leads which were unchanged from previous findings. Echo was unrevealing, however a repeat stress test showed an area of mild to moderate ischemia in the anterior wall. A subsequent coronary angiogram revealed an anomalous left coronary artery arising from the right coronary cusp. Further imaging with CT angiography showed that the anomalous coronary artery took an interarterial course with evidence of compression between the pulmonary artery and aorta. Patient was discharged with aspirin, isosorbide mononitrate, diltiazem, and nitroglycerin until scheduled patch angioplasty and reimplantation of the left coronary artery.
Discussion: It’s proposed that less than 2% of the general population have an anomalous origin of their coronary artery from the opposite sinus. In most cases, this finding is found incidentally on imaging. In cases where the artery runs an interarterial or a transseptal course, the patient may experience sudden or exercise-related cardiac death. Fibrosis is a common finding on autopsy studies, suggesting ischemia occurs prior to the terminal event. Current AHA guidelines recommend surgical intervention if there are any signs of ischemia or ventricular arrhythmias.
Conclusions: It is important to recognize congenital heart disease as a cause of chest pain in young adults as misdiagnosis can be fatal in these individuals. When symptomatic anomalous coronaries are identified, it is important to evaluate the appropriateness of surgical repair as this is the definitive management to alleviate symptoms. Patients should be counseled to restrict themselves from competitive sports or other strenuous activities while awaiting surgery.