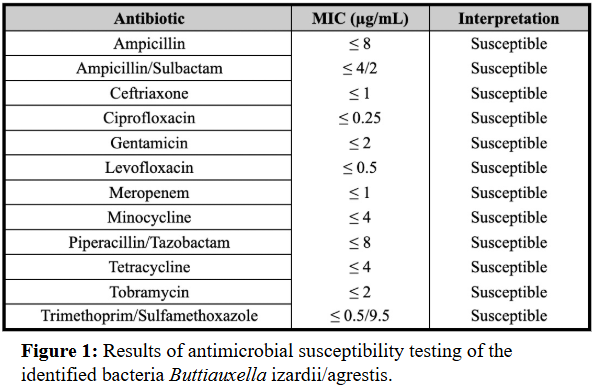
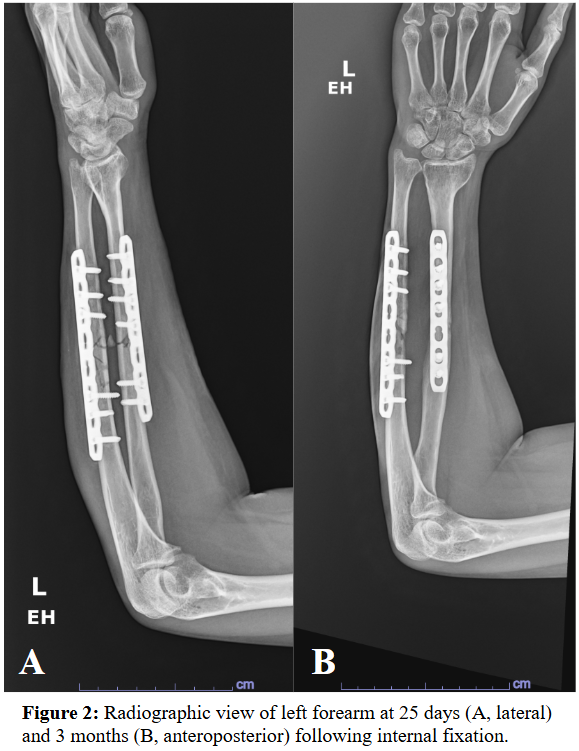
Case Presentation: A 39-year-old female with no past medical history presented 3 weeks after an ATV accident in Lebanon. She had sustained a closed left proximal humerus fracture and an open left midshaft radius/ulna fracture exposed to vegetation. She was treated in Lebanon with urgent open reduction and internal fixation, and irrigation and debridement. Ten days later, she removed her sutures and noted purulent drainage and was treated with 3 weeks of amoxicillin/clavulanate. Upon returning to the US, she was prescribed 1 week of trimethoprim/sulfamethoxazole (TMP-SMX).At initial US follow-up, the forearm had a 1 cm x 1 cm granulating wound without visible infection and mild pain along the ulnar plate with limited hand movement. Radiography confirmed stable fixation. Doxycycline was prescribed for possible deep tissue infection but declined due to GI intolerance.Five days later, she reported persistent bloody drainage. She was evaluated in the ER and scheduled for irrigation and debridement but left against medical advice despite concern for sepsis. Two days later, she returned and underwent irrigation, debridement, and sinus tract excision. Piperacillin-tazobactam and vancomycin were initiated pending cultures.Cultures grew gram-negative rod Buttiauxella izardii/agrestis, determined to be highly susceptible. She completed a 6-week course of ciprofloxacin, followed by 6 months of minocycline suppression due to retained hardware. Infection resolved; however, follow-up shows possible ulnar non-union with persistent pain requiring monitoring.
Discussion: This case represents a rare perioperative infection with Buttiauxella izardii/agrestis following ORIF of an open forearm fracture. Buttiauxella species are environmental Enterobacteriaceae and exceptionally uncommon human pathogens. Prior reports describe soft tissue or obstetric infections; involvement of retained orthopedic hardware is novel and clinically significant.Failure of amoxicillin-clavulanate reflects resistance mediated by inducible class C β-lactamase (BUT-1), analogous to AmpC enzymes in Citrobacter and Enterobacter (Fihman, Pitondo), conferring resistance to aminopenicillins and early-generation cephalosporins and reinforcing the need for comprehensive susceptibility testing in complex postoperative infections.Successful management required repeated surgical debridement and ciprofloxacin, supported by prior reports of fluoroquinolone efficacy against AmpC-producing Enterobacterales (Tamma) and B. agrestis susceptibility (Antonello). This course underscores the importance of early microbiologic identification and rapid transition to culture-directed therapy. Delayed optimization may prolong hospitalization, increase procedural burden, and heighten sepsis risk.From a hospitalist and systems-level perspective, this scenario highlights the role of early escalation protocols, antimicrobial stewardship, and multidisciplinary coordination among surgery, infectious disease, and care management to improve safety, efficiency, and quality metrics.
Conclusions: This case highlights the clinical significance of Buttiauxella infection in retained orthopedic hardware and the challenges posed by its resistance profile. Early pathogen identification and targeted antimicrobial therapy are central to minimizing morbidity and optimizing inpatient outcomes in complex trauma-related infections.