Background: Cross-cover is defined as caring for hospitalized patients for whom one is not the primary provider. This is a common, daily practice for residents and hospitalists. It has been demonstrated that the primary intern for a patient is available for only 39% of a patient’s hospital stay. Despite this, no guidelines currently exist regarding best practices of cross-coverage. Our objective was to define key components of cross-cover care using a Delphi analysis with input from hospitalists, surgeons, and chief residents that had either extensive cross-cover experience and/or educational leadership roles.
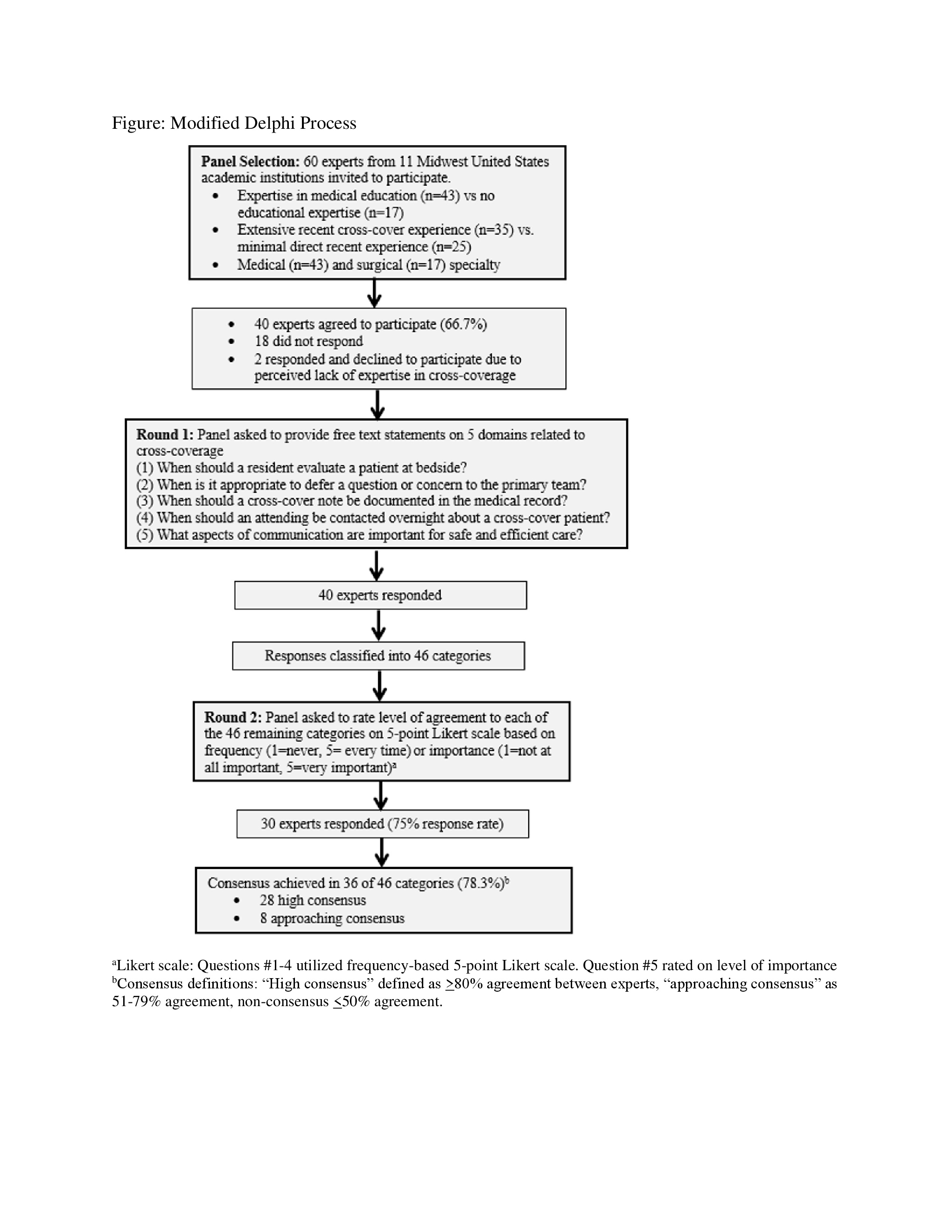
Methods: Sixty experts were invited to participate in a Delphi study in 2017 that addressed the judgment of cross-covering residents in five areas: (1) When should a cross-cover patient be evaluated at bedside? (2) When it is appropriate to defer an issue to the primary team? (3) When should a cross-cover note be documented? (4) When should a resident contact an attending overnight about a cross-cover issue? (5) What are principles of effective communication with nurses about cross-cover issues? The first survey consisted of free-text questions. Responses were categorized based on themes. In the second survey, experts rated categorized responses using a 5-point Likert scale based on appropriateness. “High consensus” was defined as >80% agreement amongst experts, “approaching consensus” as 51-79% agreement, and “non-consensus” <50% agreement. Results were analyzed by specialty (medicine vs. surgery) and cross-cover experience (none vs. any) using a Pearson chi-squared or Fisher’s exact text.
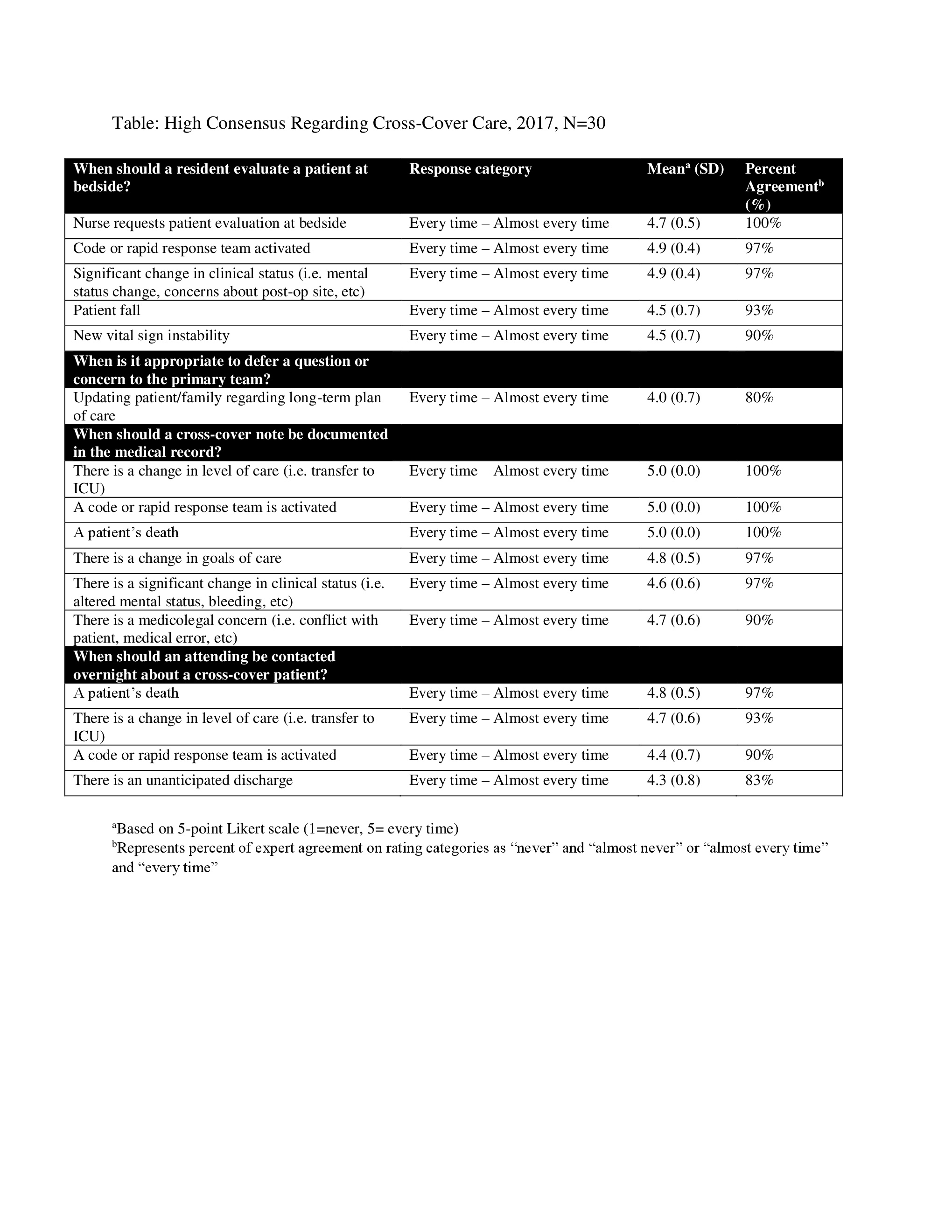
Results: Forty respondents completed the first survey (response rate 66.7%) and 30 completed the second. Responses led to 46 categories amongst the five domains; twenty-eight (60.1%) achieved high consensus (Table), eight (17.4%) approached consensus, and ten (21.7%) did not achieve consensus. There was no difference based on medical versus surgical specialty or cross-cover experience.
Several items achieved 100% consensus: residents should evaluate a patient at bedside whenever asked by the nurse; documentation should occur for change in level of care, death, a code, or when the rapid response team is activated; physician-nurse communication should be respectful and closed-loop.
Conclusions: This is the first set of guidelines that address cross-cover care. Adoption of these guidelines will help to promote uniform delivery of care. Next steps include implementation of these guidelines in our medical school and residency curriculum and evaluation of the impact.