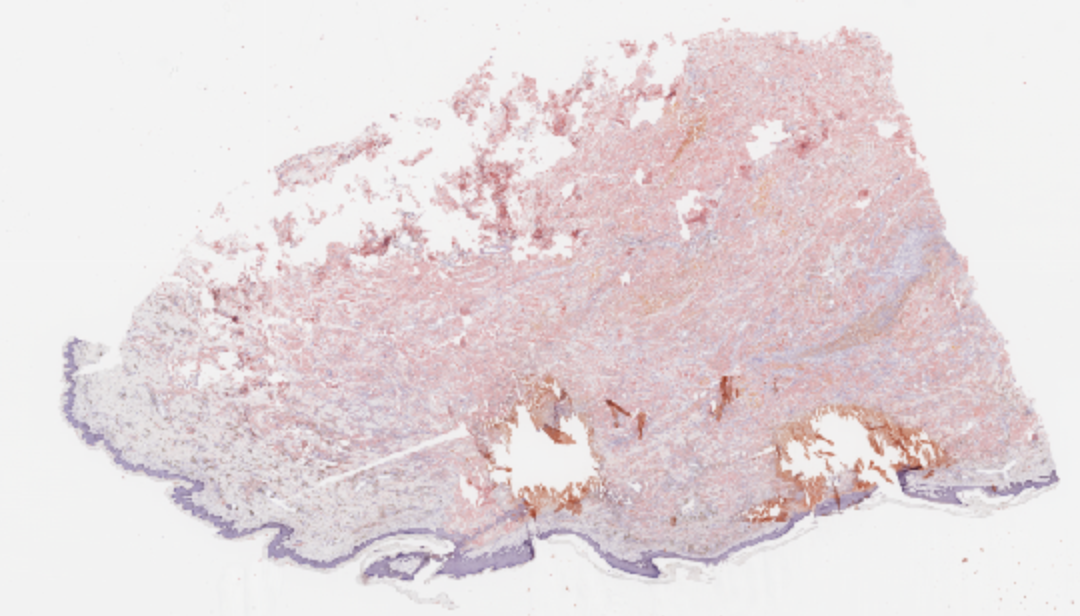
Case Presentation: A 63-year-old female with insulin-dependent diabetes was transferred to our hospital for surgical evaluation of a large, ulcerated nodule on her abdomen. The patient had been injecting insulin into the same area on her abdomen for years, causing a nodule to enlarge insidiously over past decades. It ulcerated about two years ago and eventually burst open, prompting her presentation to the hospital. The patient denied fever, chills and pain. Physical examination revealed a non-tender, firm, hyperpigmented swelling with central-draining ulceration on the left lower abdomen. Non-contrast CT of the abdomen/pelvis revealed a prominent superficial open wound with extensive soft tissue inflammation in the inferior aspect of the pannus. Punch biopsy revealed deposits of dull, pink globular material throughout the dermis. Green birefringence on polarization with Congo red stain suggested amyloidosis. Broad-spectrum antibiotics were prescribed for concurrent abscess, and excision of the infected amyloidoma was performed. The patient was ultimately discharged on oral antibiotics to complete a 14-day course.
Discussion: While the first case of insulin-induced amyloidosis was reported in 1983, the diagnosis remains relatively rare and often unrecognized. Prevalence of amyloidoma is increasing as prescriptions of insulin and other injectables become more common. Risk factors include repeated injections at the same site and the concomitant immobility or diminished manual dexterity that necessitates same site injections. Comorbidities such as immunosuppression and CKD may have been contributing factors in this case. Ultrasound (POCUS) and biopsy are useful diagnostic tools for suspected amyloidomas, as the differential diagnosis includes atypical infection, lipodystrophy, calciphylaxis, foreign body reaction or metastases. Glycemic control becomes sporadic when insulin is injected into an amyloid mass. Both hypo- and hyperglycemia have been described. Trapping of insulin within the “insulin ball” may cause insulin doses to be titrated up unwittingly in response to hypoglycemia. Amyloidosis from non-insulin injectables such as synthetic GLP-1 agonists has also been reported.
Conclusions: This case demonstrates the progression of an insulin-induced amyloidoma and emphasizes the importance of early recognition before complications ensue. Insulin amyloidomas are often underdiagnosed or misdiagnosed and may be increasing in prevalence. With increasing use of insulin and newer injectable medications such as GLP1 agonists, it is imperative that hospitalists: a) recognize and manage the complication of amyloidoma before abscess formation occurs, b) understand diagnostic and management options of amyloidomas, c) understand the consequences of repeated same-site injections and d) educate patients on the importance of rotating injection sites.