Background: Use of dexamethasone in pediatric patients with asthma exacerbations in the emergency department and ambulatory care settings has been supported in the literature as an alternative to prednisone with equivalent efficacy and potential benefits of increased compliance and decreased side effects. However, there is limited understanding of its efficacy in patients with status asthmaticus requiring hospitalization, which has led to variation and inconsistency in prescribing practices. This study aims to identify specific patient and institutional factors that influence the decisions of pediatric hospitalist attendings when prescribing prednisone (pred) or dexamethasone (dex) to treat status asthmaticus in hospitalized patients.
Methods: A survey was developed from focused interviews and was sent to the providers in the Section of Pediatric Hospital Medicine at an academic medical center. It assessed opinions on prescribing dex, and opinions on the preferred steroid based on patient factors, and institutional factors. The influence of patient factors was analyzed with Cohen’s kappa statistic and institutional factors were analyzed with a single sample χ2 test.
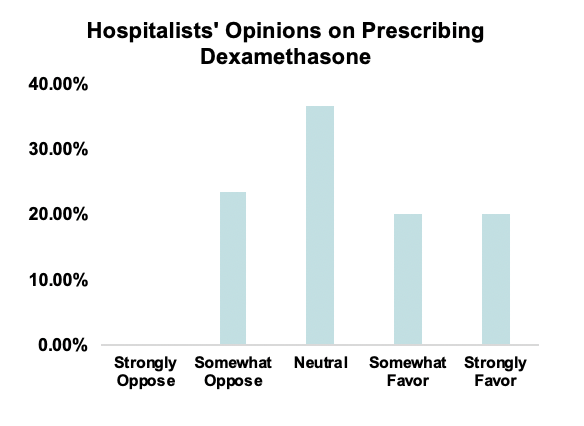
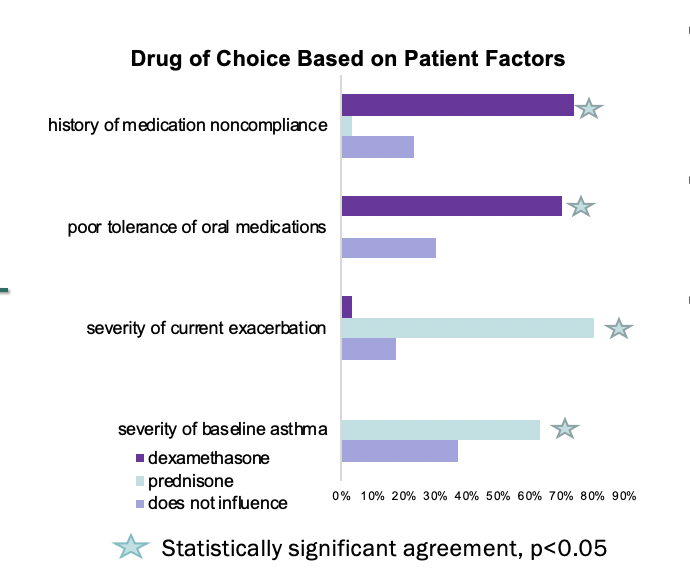
Results: 35 out of the 39 hospitalists completed the survey. Hospitalists reported wide disagreement regarding the use of dex, with 40% in favor, 36%, neutral, and 23% opposing. Moderate agreement between hospitalists was found regarding the decision to prescribe dex for patients with poor oral tolerance or a history of medication noncompliance (κ=0.520, p<0.002). There was also moderate agreement between hospitalists regarding the decision to prescribe pred for patients that have a higher severity of baseline asthma or a more severe current exacerbation (κ=0.537, p<0.0005). Hospitalists were significantly more likely to agree with the use of pred due to lack of availability of dex at community pharmacies, (χ2=10.667, p=0.005). Whether the emergency department already provided the second dose of dex and the ease of the 2-day course of dex did not significantly influence their prescribing practices (p>0.05).
Conclusions: Pred is preferred for patients with severe cases of asthma, suggesting that pediatric hospitalists are less likely to deviate from the standard treatment, possibly due to the lack of evidence of using dex for hospitalized patients. There was not significant agreement regarding the ease of the dex course as an influential factor. However, a history of poor oral medication tolerance or medication noncompliance significantly impacted their decision to prescribe dex. This suggests that currently dex is mainly prescribed as an alternative to pred when there are patient factors that conflict with the use of pred. The lack of agreement as to whether hospitalists should continue the emergency department’s second dose of dex or to replace with a course of pred demonstrates that there is not a consensus as to whether the evidence supporting the use of dex in emergency department settings can be extrapolated to the inpatient setting.