Background: At the onset of the coronavirus 2019 (COVID-19) pandemic, asthma exacerbations reportedly decreased overall, raising the question if in contrast to other viruses, SARS-CoV-2 infection does not induce asthma exacerbations1,2. Like other viruses including endemic coronaviruses, there is theoretical risk of developing bronchospasm in response to viral infection with SARS-CoV-2 for patients with a known diagnosis of asthma. Our aim was to determine the clinical characteristics of SARS-CoV-2 infection in patients with a history of asthma and incidence of bronchospasm as a marker for asthma exacerbation in response to infection with SARS-CoV-2.
Methods: This was a retrospective chart review study that characterized if infection with SARS-CoV-2 was associated with bronchospasm as a marker for asthma exacerbation in patients 2-18 years of age with a recorded history of asthma per International Classification of Disease, Tenth Revision code and a diagnosis of COVID-19 by nasopharyngeal swab. Patients were admitted to a tertiary care children’s hospital in Miami, Florida between 4/2020 to 1/2022. Institutional board review approval was obtained. Descriptive statistics were used for demographic and clinical characteristics. A chi squared test was used to test the association between bronchospasm and body mass index as well as between bronchospasm and the presence of co-infections in patients with a recorded respiratory pathogen panel.
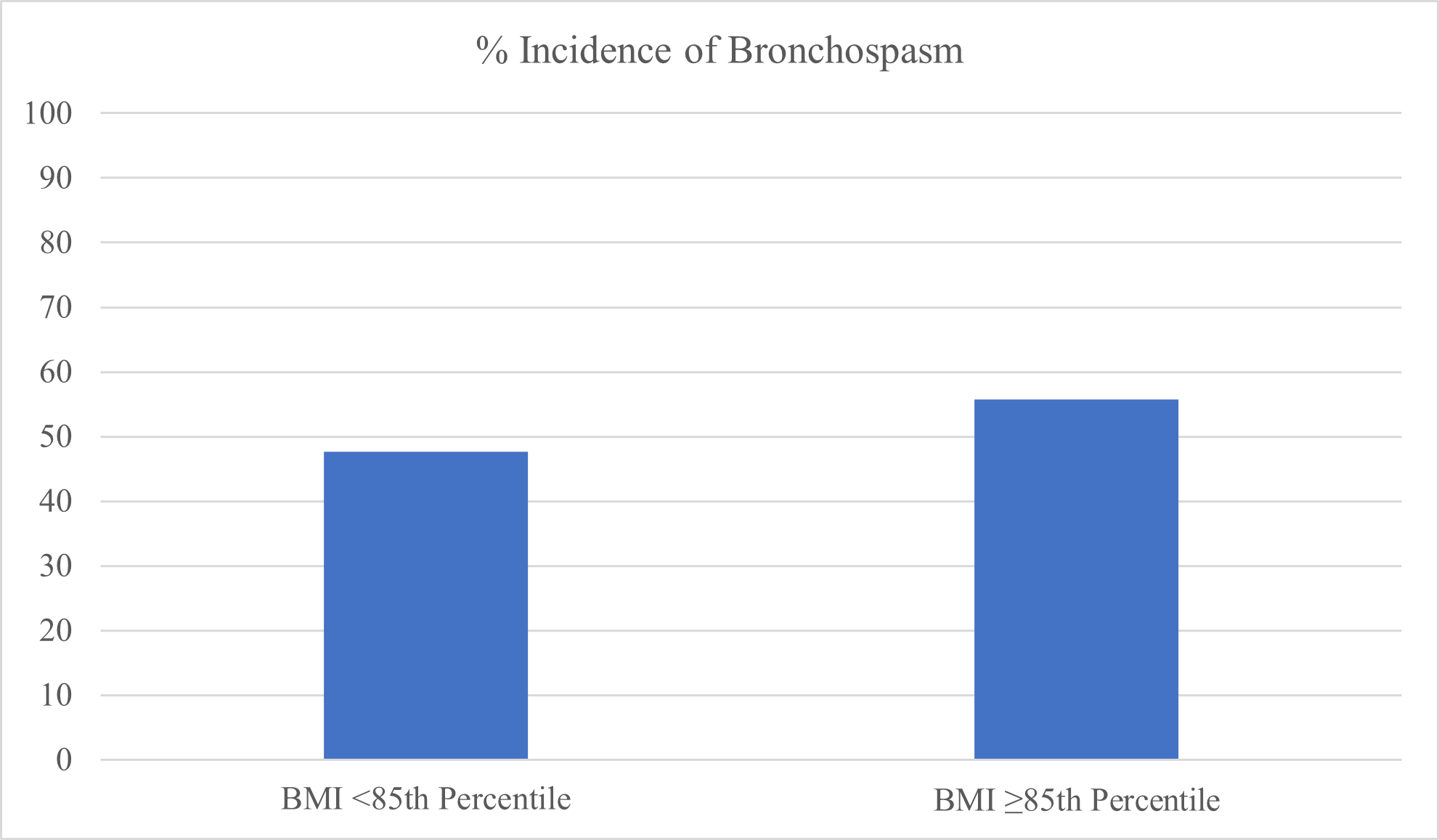
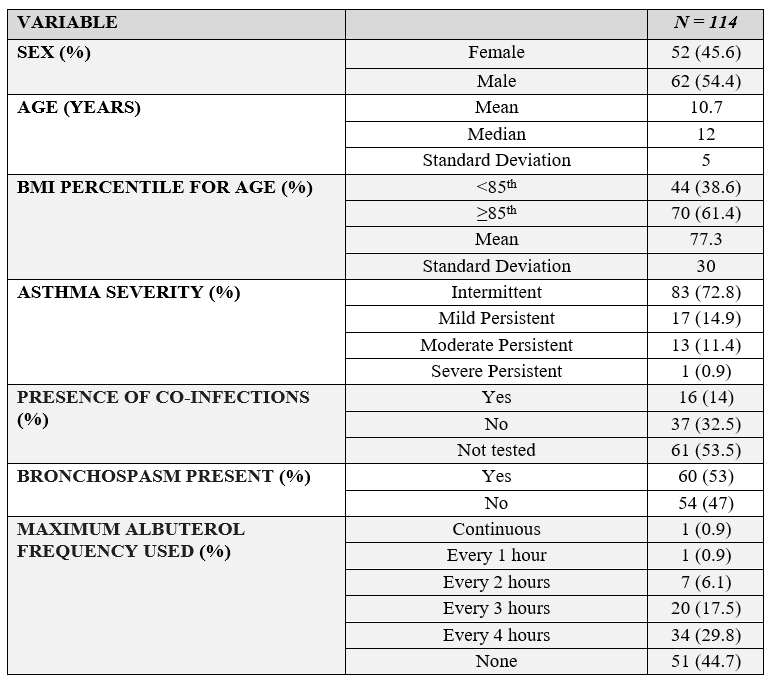
Results: One-hundred and fourteen children with a history of asthma were diagnosed with symptomatic COVID-19 requiring admission. Sixty patients developed bronchospasm in response to infection (53%), and 63 patients required albuterol and steroids (55%) (Table 1). There were 39 patients (62%) with a body mass index (BMI) greater than or equal to the 85th percentile, indicating overweight or obese body habitus. Comparing patients with BMI greater than the 85th percentile with the incidence of bronchospasm, results were not significant (p = 0.41). However, among patients with a BMI greater than or equal to the 85th percentile, there was a higher percentage of patients with documented bronchospasm compared to those with BMI less than the 85th percentile. Around 56% of patients with overweight or obese body habitus experienced bronchospasm compared to 48% of patients with BMI within normal range for age, resulting in an 8% difference (Figure 1). There was no significant difference in presence of bronchospasm in response to solitary SARS-CoV-2 infection compared to coinfection with multiple other viruses (p = 0.12).
Conclusions: Isolated SARS-CoV-2 infection may indeed be associated with bronchospasm and subsequent development of an asthma exacerbation in patients with a known asthma history, in contrast to initial beliefs. Increased BMI was not significantly associated with bronchospasm; however, patients with a BMI greater than or equal to the 85th percentile experienced more frequent bronchospasm in response to SARS-CoV-2 infection than their counterparts with normal BMI for age. With decreasing isolation measures and increased unmasking, asthmatic children remain inevitably exposed to COVID-19 and should be cautioned appropriately.