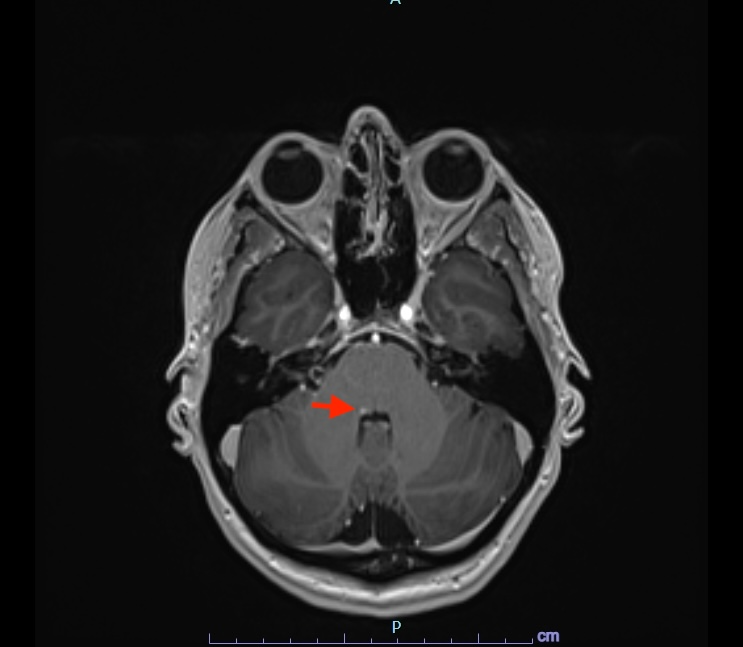
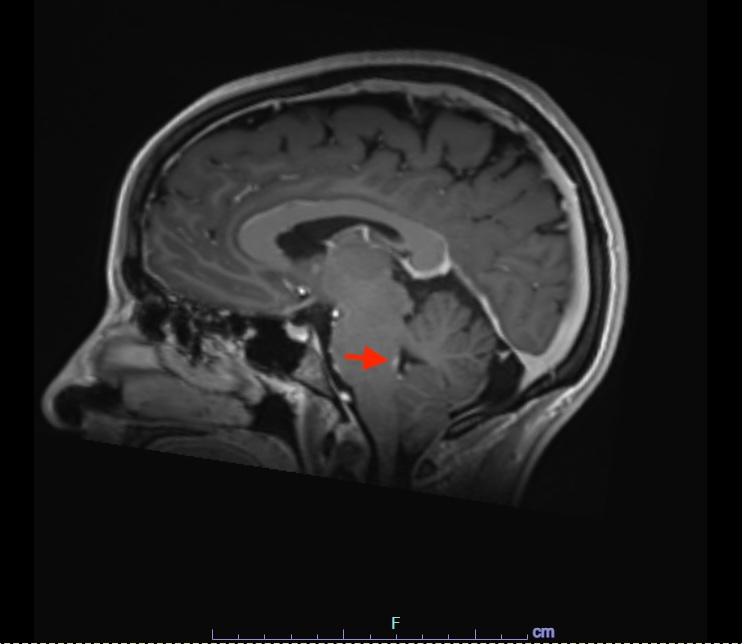
Case Presentation: A 38-year-old woman with known Behçet’s disease (BD) on hydroxychloroquine presented with six days of horizontal binocular diplopia on rightward gaze, resolving when either eye was closed. There was no diplopia on left gaze, headache, or other neurologic symptoms. Examination revealed isolated right abducens nerve (cranial nerve VI) palsy. Laboratory evaluation, CT head, and CT angiogram were unremarkable. MRI brain and orbits with contrast demonstrated a focal T2/FLAIR hyperintensity with enhancement in the posterior right pons at the level of the facial colliculus, corresponding to the right abducens nucleus (Figures 1–2). Cerebrospinal fluid analysis was normal with no oligoclonal bands; serum anti-MOG and aquaporin-4 (NMO) antibodies were negative, effectively ruling out multiple sclerosis and neuromyelitis optica. The patient received intravenous methylprednisolone (1 g/day for 5 days), leading to full resolution of diplopia by day 4. She was discharged on a tapering course of oral prednisone over one month and remained symptom-free at three-month follow-up. A nine-month MRI demonstrated complete resolution of the prior pontine lesion.
Discussion: Neurologic involvement occurs in fewer than 10% of patients with BD, most commonly as parenchymal neuro-Behçet’s disease (NBD) affecting the brainstem, spinal cord, or periventricular white matter. Brainstem involvement often manifests with ophthalmoparesis, cranial neuropathies, or cerebellar and pyramidal signs; isolated cranial nerve palsy is distinctly uncommon. Lesions typically appear T2/FLAIR-hyperintense, often with contrast enhancement during the acute phase, reflecting perivenular inflammation and small-vessel vasculitis.In this case, the lesion localized precisely to the abducens nucleus, explaining the isolated lateral rectus weakness. The differential diagnosis included multiple sclerosis, neuromyelitis optica, ischemic or infectious brainstem lesions, and venous sinus thrombosis. MRI findings confined to the pons in a patient with established systemic BD, along with rapid corticosteroid responsiveness, supported the diagnosis of parenchymal NBD. Early recognition and prompt immunosuppressive therapy are essential to prevent recurrence or progressive neurologic disability.
Conclusions: This case illustrates isolated abducens nerve palsy as a rare initial manifestation of neuro-Behçet’s disease. Clinicians should consider NBD in the differential diagnosis of new-onset diplopia, even in the absence of active systemic disease. Timely corticosteroid therapy can lead to complete clinical and radiologic recovery.