Background:
Electronic consults (“e-consults”) are commonly used in the outpatient setting to allow subspecialists to provide documented recommendations to primary care doctors without a face-to-face patient encounter. In the inpatient setting, a consult that does not require a patient encounter is often handled via informal conversation (“curbside consult”) – the consultant is not reimbursed and the requesting physician risks patient safety by acting on undocumented recommendations. An e-consult for the inpatient setting is not well-described.
Purpose:
Design and implement a protocol for subspecialists to provide e-consults for adult inpatients at a remote site of an academic medical center.
Description:
In February 2015, our institution opened a new hospital four miles from the main medical center. The new hospital is home to several adult inpatient services, including obstetrics, urology, and colorectal surgery. A hospitalist is on-site at all times to perform consults and to serve as a liaison to subspecialty consults if the question is beyond a hospitalist scope of practice. Since subspecialists are not based at the new site, they have three options for performing consults: in-person, remote video, and e-consult.
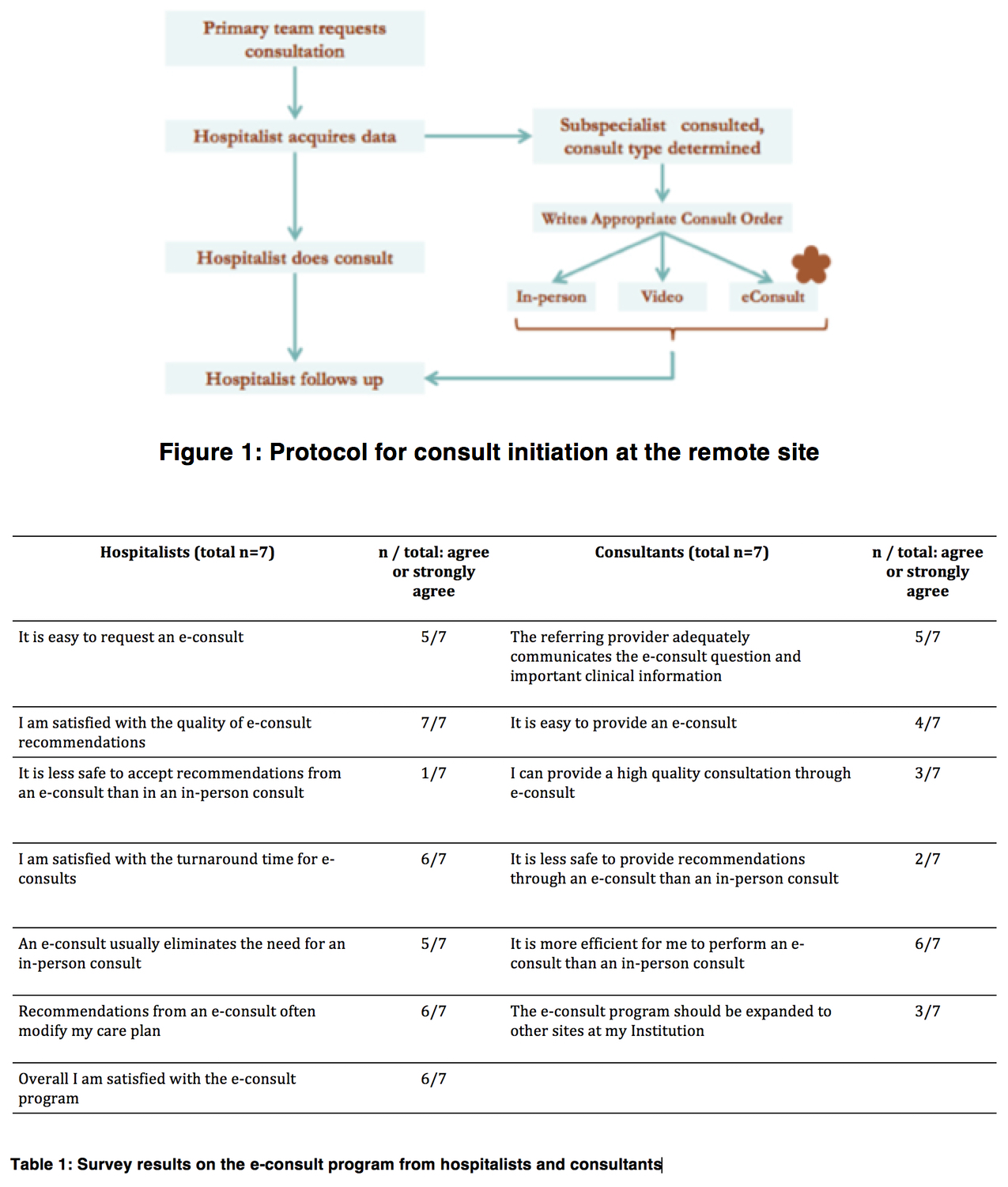
The e-consult begins with a phone call between the subspecialist and the requesting hospitalist (Figure 1). They discuss the consult question and agree on the consult modality. For e-consult, the subspecialist reviews the patient’s chart then documents in an e-consult note that is reimbursed internally by the medical center. The subspecialist can perform follow-up in any of the three consult modalities.
There have been 187 e-consults to date. The top consult services are nephrology, infectious disease, and endocrinology.
We solicited feedback from hospitalists and subspecialists who had completed at least two e-consults (Table 1). Both groups agreed that e-consults were efficient. All hospitalists were satisfied with the quality of e-consult recommendations but only 3/7 subspecialists agreed that they can provide a high-quality consultation via e-consult. Notably, only 2/7 subspecialists reported that e-consults were less safe. There have been no reported patient safety issues related to e-consults to date and a chart review of all e-consults during the first three months of the program found no significant safety issues.
Conclusions:
An inpatient e-consult program is a practical method for providing formal subspecialty consultation to a remote hospital when a face-to-face patient encounter is not clinically necessary.