Background: While predictive analytics can help anticipate trends, the specific consequences of a national disaster on the healthcare system are often unpredictable. Recently, the East Coast suffered supply chain disruptions due to hurricane damage, leading to dramatic shortages of saline, intravenous (IV) fluids, and dialysate. The damage to Baxter’s North Carolina facility, which represents 60% of the U.S. IV fluid market and serves 36 countries internationally, forced healthcare systems nationwide to immediately implement measures to ensure continuity of patient care and safety. These efforts echoed those from the early and intense months of the pandemic.
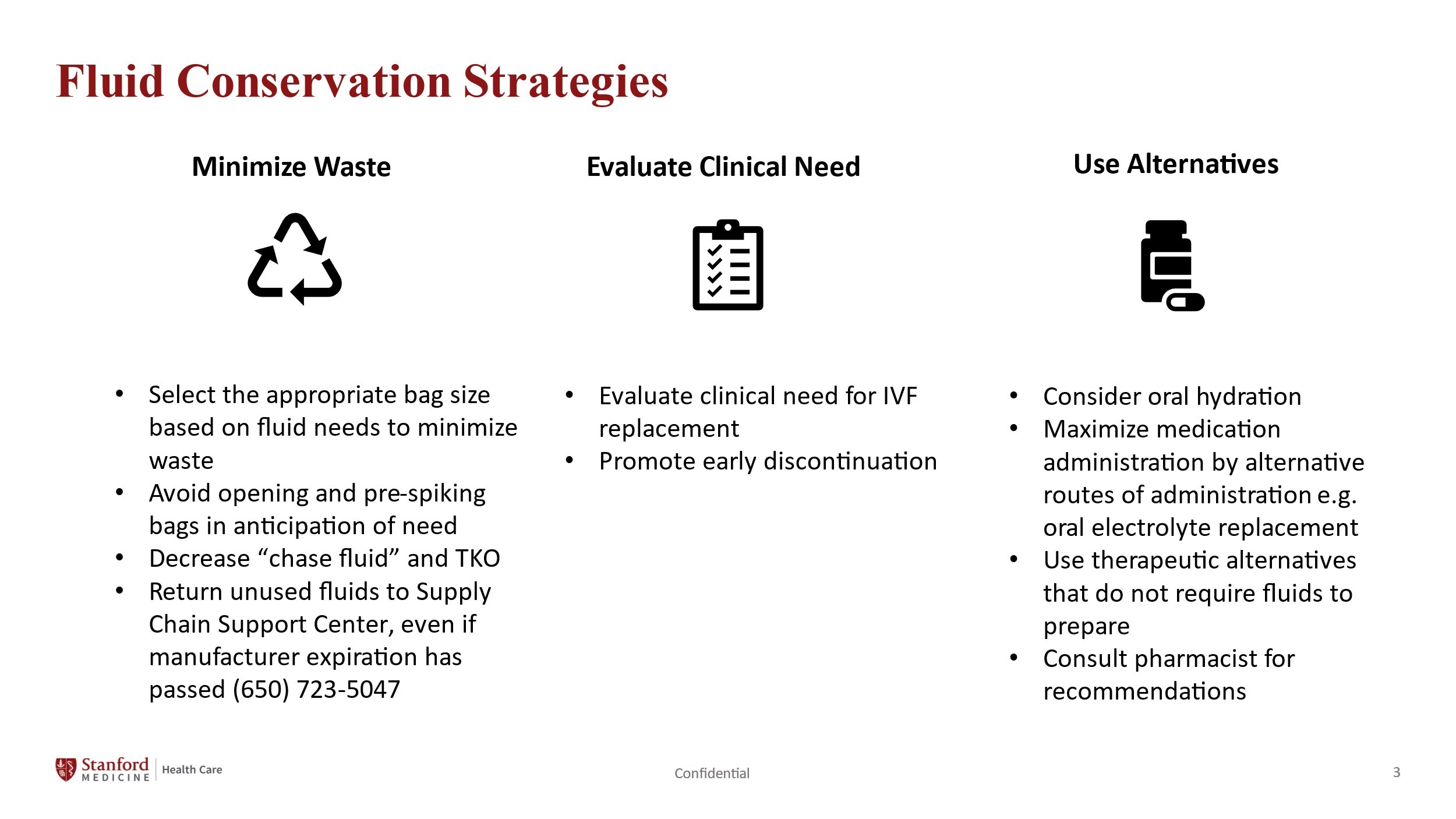
Methods: Hospitals have rapidly developed comprehensive conservation measures, focusing on minimizing waste and ensuring continued patient care during an unknown duration of limited resources. At our institution (a 600+ bed, quaternary academic medical center), we utilized a five-level strategic management framework—Predict, Prevent, Prepare, Respond, and Recover. These efforts were guided by partnerships, governance, and intelligence to ensure supply chain resiliency. A multidisciplinary task force convened multiple times weekly to mitigate organizational risk by identifying, reviewing, and approving clinically acceptable alternatives. We used a data-driven approach to monitor IV fluid usage and assess burn rate to identify the fluids at highest risk of depletion and the associated departments who used the specific fluids the most. Continuous real-time assessments and root cause analyses of deviations were conducted to optimize these protocols. EMR-generated hard stops on IV fluid maintenance infusions, best practice alerts, and nursing/pharmacy cues helped curb excessive IV fluid ordering on each patient. Ethicists helped ensure the processes were fair and equitable along the way and impart the principles of procedural justice.
Results: The implementation of system-wide conservation measures demonstrated the potential for many strategies to become permanent best practices. Monitoring our fluid use provided clear insights into the departments with the highest utilization of IV fluids, such as ICU, Surgery, Pediatrics, and Pharmacy, enabling focused conservation efforts. We presented visuals on a regular basis to clinicians across the organization and to medical leaders to help the teams minimize waste and implement standardize produce usage. For example, promoting the use of premix medications and reducing in-house fluid preparation minimized waste and improved resource utilization. These measures resulted in significant cost savings and labor efficiency while ensuring continuity of care. Collaborative workflows allowed rapid implementation and reduced unwarranted variation, supporting sustainability efforts.
Conclusions: Natural disasters and pandemics demonstrate the need for strong governance, agile responses, and multidisciplinary collaboration in supply chain management. This crisis highlights the importance of adopting a zero-waste approach, including real-time data utilization and conservation strategies. By preserving these innovations as long-term best practices, healthcare systems can evolve into more sustainable organizations. The return on investment of labor time, saved supplies, and improved efficiency compels healthcare systems to reevaluate and improve existing workflows.