Case Presentation: A 45 year old AA Male with PMHx of hypertension and ESRD on HD for 10 years with severe (8/10), diffuse epigastric pain associated with nausea, vomiting, high fever and chills for 2 days. ROS was positive for bloody diarrhea, SOB at rest, blood tinged sputum when coughing, altered sensorium and diffuse joint pain.
On exam, vitals showed Temp of 40.5, RR of 45 and HR of 124. He had diffuse tenderness in right lumbar and iliac fossa, diminished air entry in all lung fields and only oriented to self. Initial labs showed normal WBC but bandemia of 36, hgb of 7.4, platelets of 36, amylase of 881 and lipase of 817. Chest XR showed nonspecific patchy opacities in both lungs, with possibility of pneumonia. CT scan of abdomen showed periportal and peripancreatic adenopathy suspicious for haemorrhagic pancreatitis.
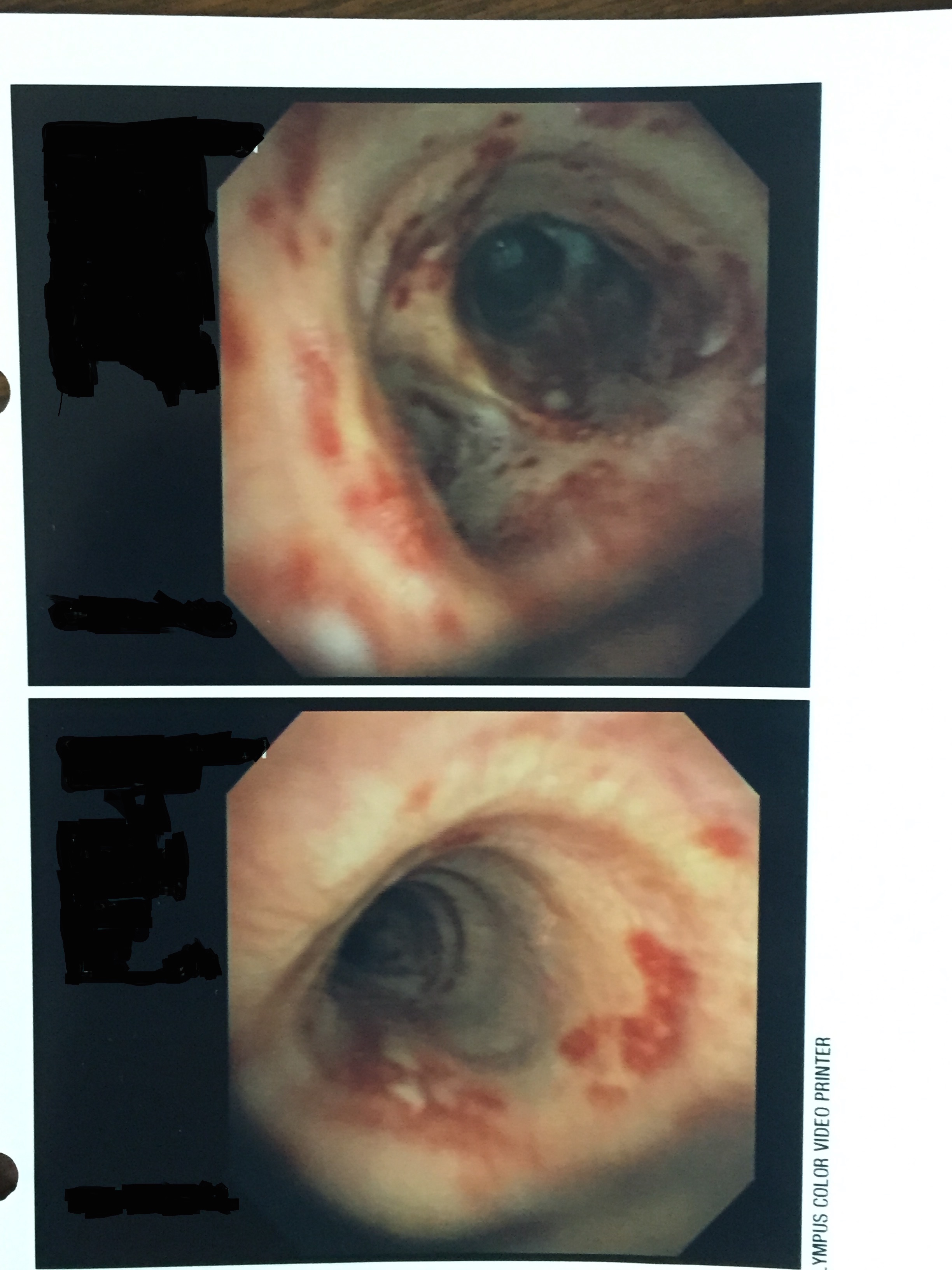
The next day, he began to desaturate and was intubated. Over the next few days, although receiving adequate fluid resuscitation and antibiotics, patient showed no improvement in condition. Echo done showed EF of 10%, a stark decrease in cardiac function as previously he had preserved cardiac function 8 months ago. Bronchoscopy was done, which showed diffuse erythematous lesions throughout bronchial tree with extremely rare haemorrhagic white plaques seen. At this point, a suspicion of vasculitis was raised and panel was sent. Results were positive ANA and ANCA, decreased C3 and C4, along with positive Anti-DSDNA and Anti- Smith Ab. Diagnosis of SLE was made and patient was treated with high dose steroids for 10 days. Patient improved rapidly and was weaned off ventilator. He was tapered on high dose steroids and mycophenolate mofetil, and was transferred to a nursing home for further rehab on his deconditioning.
Discussion: Systemic lupus is an autoimmune disease where the body’s own immune system attacks healthy tissue, causing wide range of complications ranging from vasculitis of blood vessels to accelerated atherosclerosis. The prevalence of SLE is between 20-50/100000 with AA Female by far the most affected populated subgroup. Though SLE incidence is relatively high, improved detection has resulted in appropriate care being delivered in a timely manner, resulting in manageable long term prognosis. Acute disseminated SLE is extremely rare, with very few reports seen, but should be considered in a septic patient who does not improve despite receiving appropriate care.
Conclusions: Vasculitis is generally a diagnosis of exclusion, but one that should be considered when common management fails to lead to clinical improvement. Broad presentations of acute thrombocytopenia, reduced cardiac function, interstitial inflammation leading to fibrosis and intra alveolar hemorrhage, and psychosis are all possible variances of how disseminated lupus may appear. Timely diagnosis of treatment with high dose steroids brings remarkable reversal of symptoms, thus essential in early detection to prevent morbidity and mortality for the internist.