Background: The 2015 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend the use of systemic corticosteroids in the treatment of acute exacerbations of chronic obstructive pulmonary disease (AECOPD). Although prior guidelines did not recommend a dose or route, current guidelines recommend oral (PO) prednisone over intravenous (IV) methylprednisolone for non-ICU AECOPD hospitalizations, given lower costs and equivalent patient-level outcomes. Prior studies have shown considerable variability in the route and dosage of corticosteroids used in the management AECOPD in both the ED and inpatient settings, despite these guidelines.
Methods: A retrospective chart review was performed of patients hospitalized for AECOPD to a 552-bed academic tertiary care medical center between September 2012 and May 2014. AECOPD hospitalizations were identified by ICD-9 billing codes. Exclusion criteria included patients who left against medical device, were admitted/transferred to ICU level care, or upon further chart review were not hospitalized primarily for AECOPD as judged by reviewers. Patients were analyzed in cohorts based on whether they had received IV or PO route of corticosteroid in the ED. Further subgroup analysis was performed based on whether patients required supplemental oxygen therapy on discharge.
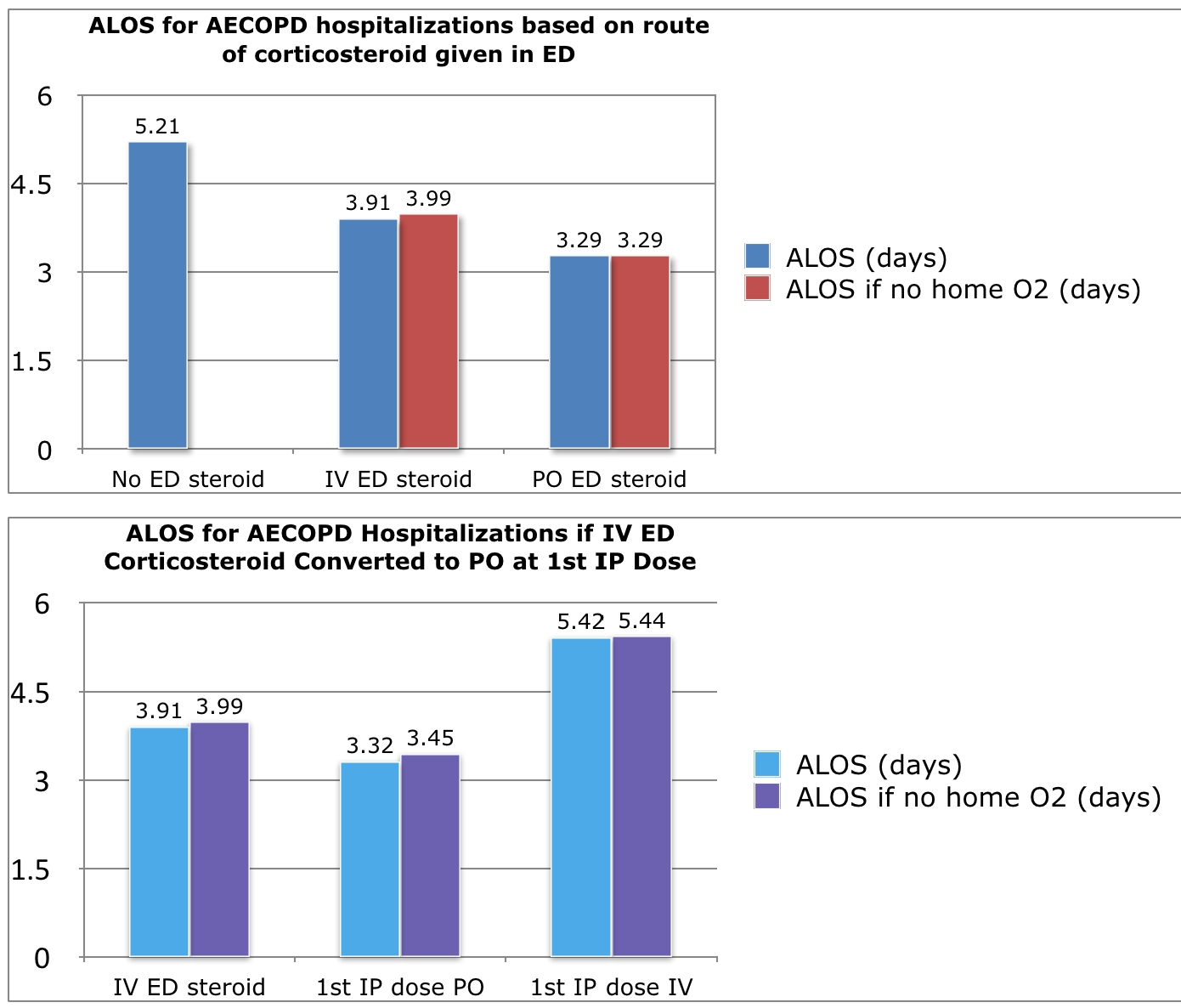
Results: Over a 20-month period, 314 AECOPD hospitalizations were identified by ICD-9 billing codes. 285 patients were analyzed after exclusion criteria were applied. Corticosteroids were not given in the ED in 19.6% (n=56) of patients, and by IV route in 45.2% (n=129) versus PO route in 35.1% (n=100). Patients receiving corticosteroids by IV route in the ED had a higher average length of stay (ALOS) compared to those who received PO corticosteroids in the ED (3.91 days vs. 3.29 days). ALOS for patients who received no ED corticosteroid was the highest at 5.21 days. When analyzing only patients who were not discharged on supplemental oxygen therapy, patients getting IV corticosteroids in the ED also had a higher ALOS compared to those who received PO corticosteroids (3.99 days vs. 3.29 days). Patients who received IV corticosteroids in the ED to but were converted to PO with the first dose in the inpatient (IP) setting, were found to have a shorter ALOS (3.32 days) compared to those who were not (5.42 days). The shorter ALOS for patients converted to the PO route immediately in the IP setting persisted when analyzing only those patients not discharged on supplement oxygen therapy (3.45 days if changed to PO on first IP dose, 5.44 days if not).
Conclusions: Intravenous administration of corticosteroids to patients hospitalized for AECOPD was associated with a higher ALOS compared to PO administration. Converting patients to PO corticosteroids immediately in the IP setting resulted in mitigation of the increased ALOS associated with IV ED corticosteroids.