Background: Current daily clinical demands significantly limit a hospitalist’s ability to proactively escalate process delays or maintain a comprehensive grasp of the entire hospital medicine census. This fragmented, non-structured communication, particularly at the inter-departmental level, fails to address timely, system-wide resolution of bottlenecks. While traditional throughput models (e.g., Discharge Hospitalist, Nurse-Led Flow Coordination) have shown efficacy, they either focus too narrowly on discharge logistics or lack the clinical expertise needed to resolve complex, physician-dependent delays via peer-to-peer communication.
Purpose: To evaluate the impact of a novel, dedicated Throughput Hospitalist role on operational metrics by introducing structured, physician-led communication to the hospital flow process.
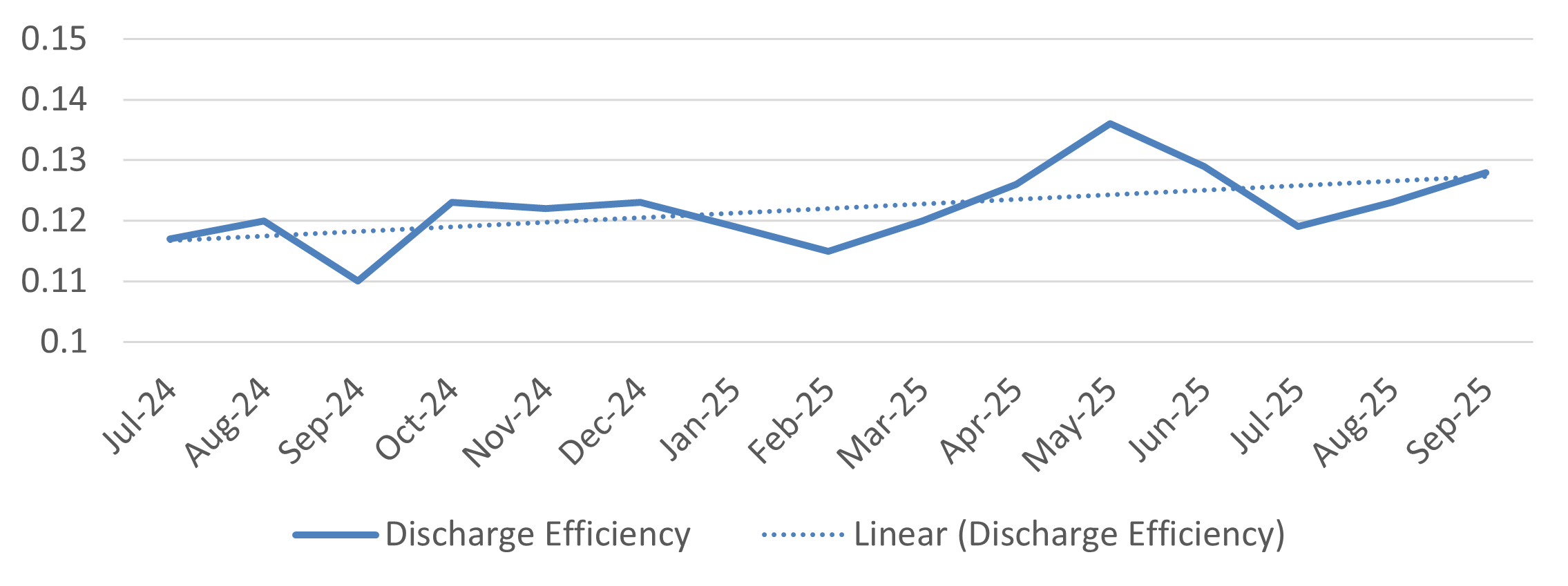
Description: This intervention was implemented at a 900-bed tertiary care academic center in November 2024. The Throughput Hospitalist is a non-clinical hospitalist dedicated solely to operational flow. Their mechanism is three-fold: 1) Utilizing physician expertise for peer-to-peer escalation. 2) Acting as a direct resource for clinical teams. 3) Establishing structured, thrice-daily throughput huddles to streamline communication and facilitate coordination with key operational partners (e.g., Leadership in Nursing, Case Management, Radiology, Interventional Radiology, Cardiac Testing, Psychiatry, Rehabilitation Services, Bed Management and Transportation, Patient Experience).We compared 12 months of pre-intervention data (11/1/2023–10/31/2024) to post-intervention data (11/1/2024–10/31/2025), focusing on the LOS Observed-to-Expected (O/E) Ratio and the monthly trend of Discharge Efficiency (ratio of daily discharges over clinical encounters). Comparison of the pre-intervention to post-intervention period demonstrated a significant improvement in efficiency (Table 1). The LOS O/E Ratio decreased from 1.18 to 1.13, representing a 0.05 absolute reduction toward the national benchmark. Furthermore, Discharge Efficiency showed a substantial positive change in slope post-intervention (Figure 1), indicating an accelerated improvement in the ratio of discharges per clinical encounter after the intervention began.
Conclusions: Our Throughput Hospitalist model is an effective innovation that resolves a core operational weakness—fragmented executive communication—by integrating a physician with operational expertise into the system to ensure effective communication at the peer level and with key hospital leadership. This adaptable model rapidly achieved significant, quantifiable flow improvements.