Background: Older adults commonly lose mobility during hospitalization. This loss of mobility may be preventable if it is identified and addressed early in a patient’s hospital course. However, currently there is no systematic method to identify these patients early, and current practices are guided by physician experience and intuition. To this end, we used machine learning algorithms to predict, on the first hospital day, a patient’s likelihood of losing mobility during their hospitalization.
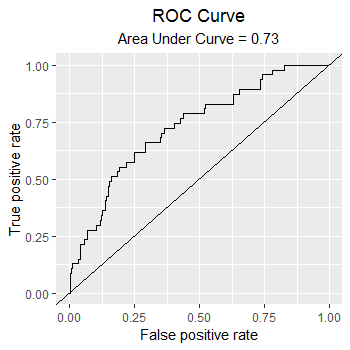
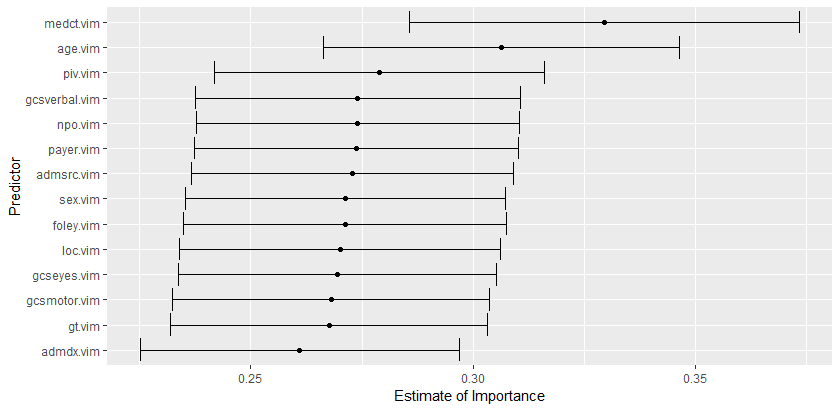
Methods: We conducted a retrospective cohort study of 2215 patients discharged from the hospital medicine service of a large academic medical center in 2018. Patients were included if they were over 65 years old and if the bedside RN charted that they were ambulatory on admission. Demographic, clinical, and functional data were extracted from the medical record. We only included predictors available on hospital day one. Loss of mobility was determined by the mobility sub-scale of the Braden Mobility Score (BMS), which is recorded twice daily by nursing staff. We created derivation and validation cohorts using an 80/20 sample approach. We employed ensemble machine learning methods to develop the prediction model. We used the SuperLearner package in RStudio (Version 1.1.463) to generate a final model using a weighted combination of statistical methods including gradient boosted trees, linear regression, and random forest. The final model was applied to the validation set to assess discrimination (Figure 1) and estimates of variable importance were calculated for each predictor (Figure 2).
Results: No difference in baseline characteristics existed between the derivation and validation groups. The mean age was 77 years, most patients were female (51%), and most were admitted through the Emergency Dept (85%) to an Acute Care bed (71%). Of the 2215 patients who met the study admission criteria, 172 patients (7.8%) lost mobility and 11 patients (0.04%) were excluded because they were missing outcome data.The final model features included patient sex, age, admit source, level of care, payer class, foley status, gastric tube status, NPO status, number of medications taken, number of peripheral IVs inserted, Glasgow Coma Scale, and admission diagnosis. The final model discriminated relatively well, with a c-statistic of 0.73 (Figure 1). Estimates of variable importance were also calculated (Figure 2).
Conclusions: It is possible to predict those at risk of losing mobility using data only from hospital day one. Such a tool allows physicians to intervene early in patients at greatest risk of mobility loss and allows administrators to better allocate hospital limited therapy resources to preserve and promote mobility for inpatients.