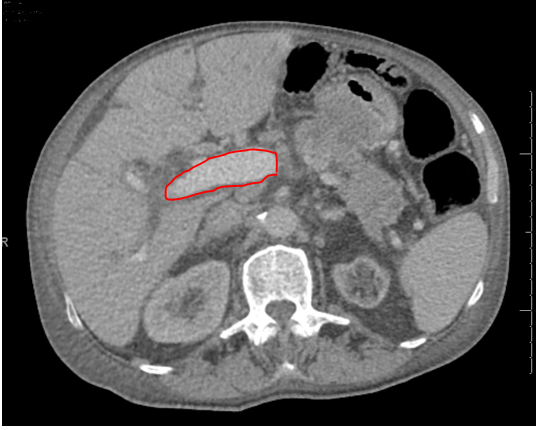
Case Presentation: An 84-year-old male with a PMH of CAD, atrial fibrillation and BPH presented to the ED due to night time vision loss and jaundice. Patient stated one month prior to presentation he noticed difficulty with vision at night while driving. One week prior to presentation, patient’s family noticed new-onset jaundice. Upon presentation, patient had a fever of 38.1°C, but was otherwise hemodynamically stable. Primary work-up showed concerns of obstructive jaundice with AST 170, ALT of 95, INR 2.69, total bilirubin of 7.3 with a direct bilirubin of 6, alkaline phosphatase of 1000 and WBC of 15.2. Patient was given appropriate vitamin K supplementation for elevated INR. Patient was started on Ceftriaxone/Flagyl for concerns of ascending cholangitis. CT abdomen/pelvis demonstrated progressive intrahepatic and extrahepatic biliary dilatation with a soft tissue mass-like area extending from the pancreatic body to the posterior gastric wall with accompanying gastric wall thickening with suspicion for malignancy. ERCP showed cholangitis due to terminal duct stricture due tumor burden, biliary sphincterotomy was done and a trans-papillary fully covered metal stent was placed in the bile duct. CA19-9 was elevated at 293.4. Biopsies of the terminal bile duct and tumor appearing tissue were obtained. Terminal bile duct biopsy and cytology revealed pancreatic adenocarcinoma. Due to suspicion of fat-soluble vitamin deficiency from malabsorption, vitamin A levels were found to be <13 (L). Ophthalmology was consulted for nyctalopia, and they recommended appropriate vitamin A supplementation for vitamin A deficiency. Patient was given IV vitamin A supplementation and discharged on oral vitamin A. Patient had appropriate Oncology follow up.
Discussion: We present a rare case of a pancreatic tumor presenting with nyctalopia from obstructive malabsorption causing vitamin A deficiency. Currently in the United States, pancreatic cancer is the 11th leading cause of cancer. Upon diagnosis, 80% of patients have unresectable masses due to its late detection and vague initial presentation [1]. Abdominal pain and jaundice are the most common presenting symptoms of pancreatic tumors [1, 2]. Malabsorption is an exceedingly rare presenting sign [2]. Malabsorption can occur due to lack of pancreatic enzymes leading to steatorrhea with loss of fat-soluble vitamins. Vitamin A is a fat-soluble vitamin that is essential to many physiologic functions, especially vision. It is necessary for the production of visual pigments in the rods and cones, photo signal transduction and the maintenance of the corneal and conjunctival epithelium [3]. Night vision loss is often one of the first symptoms of Vitamin A deficiency as seen in this case [3]. Untreated Vitamin A deficiency can lead to permanent blindness. In developing countries, it is a common cause of blindness [3]. There are, however, rare reported cases of Vitamin A deficiency occurring in developed countries after bariatric surgery, pancreaticoduodenectomy, and chronic pancreatitis [3-5]. The mechanism of malabsorption occurs from lack the pancreatic enzyme, lipase, necessary for lipid reduction to allow for absorption and transport of Vitamin A [3].
Conclusions: Nyctalopia can be a very rare presentation of pancreatic mass, resulting from malabsorption from obstruction and lack of pancreatic enzymes. There are few documented cases of a pancreatic tumor presenting with Vitamin A deficiency [6-8], making this is an exceedingly rare presentation of pancreatic tumor.