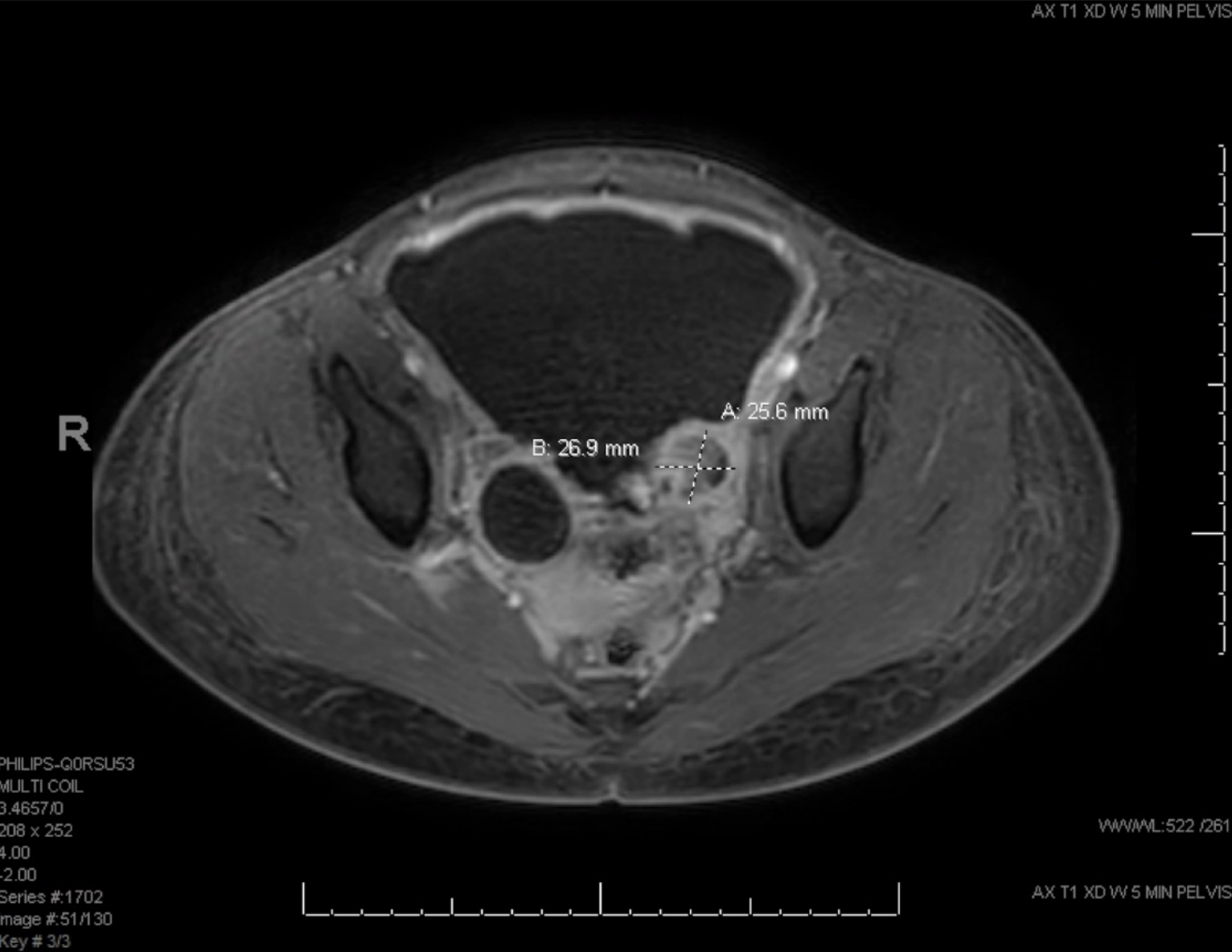
Case Presentation: A 13-year-old South Sudanese female with poorly controlled Type 1 Diabetes presented to the emergency department with one month of progressive abdominal distention. She presented twice previously to an urgent care with an unremarkable evaluation and had temporary improvement with polyethylene glycol, but her abdominal distention and intermittent pain worsened. She denied fevers, chest pain, emesis, diarrhea, upper respiratory symptoms, bleeding, or bruising. Vital signs were normal for age. Physical exam was remarkable only for a significantly distended, firm, non-tender abdomen, with no obvious masses palpated. Complete blood count, metabolic panel, lipase, procalcitonin and urine studies were unremarkable. CT scan of the abdomen showed substantial ascites with omental caking, suspected peritoneal nodules in the pelvis, and findings consistent with malignancy. Pelvic ultrasound revealed no left ovarian tissue, but amorphous tissue with blood flow likely representing a tumor. She was admitted to the Oncology service for further workup of a presumed ovarian malignancy. Ovarian tumor markers were normal (β HCG, AFP and LDH) except for elevated CA-125 (87 U/mL). MRI demonstrated a left ovarian mass with restricted diffusion and post-contrast enhancement consistent with a neoplasm (Figure 1). Pediatric surgery was consulted and performed a therapeutic paracentesis. Diagnostic laparoscopy revealed a diffuse intra-peritoneal process with studding on all peritoneal surfaces and a firm left ovarian mass containing pus. Biopsies were obtained from the peritoneum, omentum, and ovarian mass. To minimize surgical time, concurrent port placement was strongly considered for anticipated chemotherapy; however, upon multidisciplinary discussion this was deferred pending the final diagnosis. Pathological evaluation of tissue ultimately revealed granulomatous inflammation with coccidioides organisms in all specimens and no evidence of malignancy. She was transferred to the Hospitalist team, and Infectious Disease was consulted for management of disseminated peritoneal coccidiomycosis. Her serum coccidioides antibody titer was 1:256, but bone scan and lumbar puncture were negative. Due to the severity of her surgical findings, she was treated with two weeks of IV amphotericin B in combination with oral fluconazole for long-term management.
Discussion: Coccidiomycosis, also known as Valley Fever, is a common fungal infection in the Southwestern United States. It typically presents as a self-limiting, often asymptomatic, pulmonary infection. However, in patients who are immunosuppressed, or those of African or Filipino ancestry, the risk of disseminated, extrapulmonary disease is much higher. This patient was at particularly high risk for dissemination given her ancestry and immune deficiency secondary to uncontrolled Type 1 Diabetes. There was significant anchoring bias early on in this case, evidenced by the patient’s initial admission to the Oncology service and consideration of a port prior to a confirmed diagnosis. Multidisciplinary team discussion in this case was critical to the avoidance of an ultimately unnecessary procedure.
Conclusions: Maintaining a broad differential and awareness of local endemic diseases, as well as associated risk factors, is critical for prompt workup and diagnosis of rare disease presentations. Intrinsic to this is avoiding anchoring bias to explore further diagnostic possibilities, while avoiding unnecessary invasive interventions.