Background: Patients with cirrhosis complicated by ascites are often admitted to the hospital and require abdominal paracentesis for diagnostic evaluation and symptom relief. When large volumes are removed there is a risk for acute kidney injury (AKI) which can contribute to morbidity and mortality. There are no clear guidelines for what constitutes a safe volume for removal while patients are in the hospital
Methods: This retrospective cohort study sought to evaluate the association between the volume removed during a therapeutic paracentesis and the risk of developing acute kidney injury during hospitalization. Patients 18 years and older who were referred to the internal medicine bedside procedure service for therapeutic paracentesis of at least 500 milliliters between 9/1/2015 and 9/1/2018 were included. Patients who were on dialysis prior to paracentesis or who were admitted for renal failure were excluded as were patients that did not have a baseline creatinine within 48 hours of the procedure and those that did not have at least one follow up creatinine within 7 days of the procedure. Patients with ascites not due to cirrhosis or portal hypertension were also excluded from analysis. AKI was defined using the KDIGO guidelines with the definition of AKI being met for a 0.3mg/dL or greater rise in creatinine within 48 hours or an increase in serum creatinine by 1.5 times or greater within 7 days. Other factors relevant to the clinical history were also evaluated in our model including INR, MELD, GI bleeding, sepsis, peritonitis, and exposure to diuretics
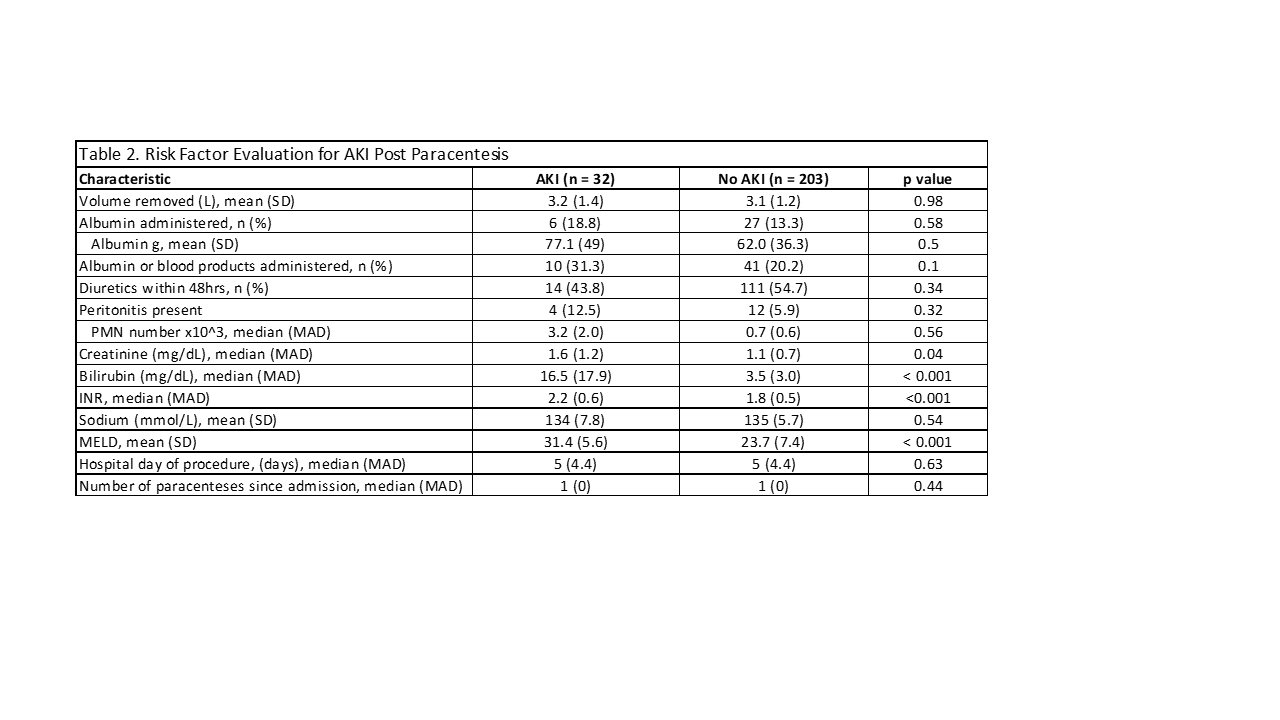
Results: A total of 516 therapeutic paracentesis were performed during the study period. We excluded 130 which were performed on patients without liver disease, 120 which were performed on patients receiving dialysis, 14 with less than 500 milliliters removed, and 17 with AKI preceding paracentesis. Our final sample included 235 therapeutic paracenteses that were performed in a cohort of 84 unique patients. Thirty-two paracenteses (13.6%) were associated with an acute kidney injury as defined by the KDIGO criteria. The MELD score, creatinine, bilirubin and INR were identified as risk factors for the development of AKI (odds ratios of 7.2 (3.3; 16.1), 3.1 (1.4;6.7), 5.1 (2.4;11.2) and 5.7 (2.1;15.3), respectively). Whereas there was no association with volume removed (mean(sd): 3.1L(1.3)) and the development of acute kidney injury
Conclusions: In this cohort of hospitalized patients with cirrhosis undergoing therapeutic paracentesis we did not observe an association between the volume removed and the development of AKI. However, the MELD score was identified as the most significant risk factor for the development of AKI along with other parameters associated with end-stage liver disease.