Case Presentation: A 14-year-old female with a one-month history of iron-deficiency anemia due to menorrhagia presented to the emergency room for weakness and dizziness. She was found to have a hemoglobin of 3.7 g/dL in the setting of her menstrual cycle. Menarche began at age 13 and has gradually become longer and heavier. Most recent menstrual cycles have lasted 7-8 days and required pad changes every 1-2 hours. Due to her severe anemia she received a red blood cell transfusion, and pediatric hematology was consulted. Initial coagulation testing was notable for PT/PTT prolonged at 20s and 46s respectively (Table 1). Coagulation testing did not correct with mix. Based on concern for an inhibitor, the patient was started on progesterone only birth control. Following discharge, she was found to have positive anti-cardiolipin, beta2 glycoprotein and lupus anticoagulant. Other than a small palatal and nasal ulcer, her exam was unremarkable. ANA was positive with a 1:2560 titer and anti-dsDNA was 448. She was diagnosed with SLE and started on prednisone, hydroxychloroquine, azathioprine.
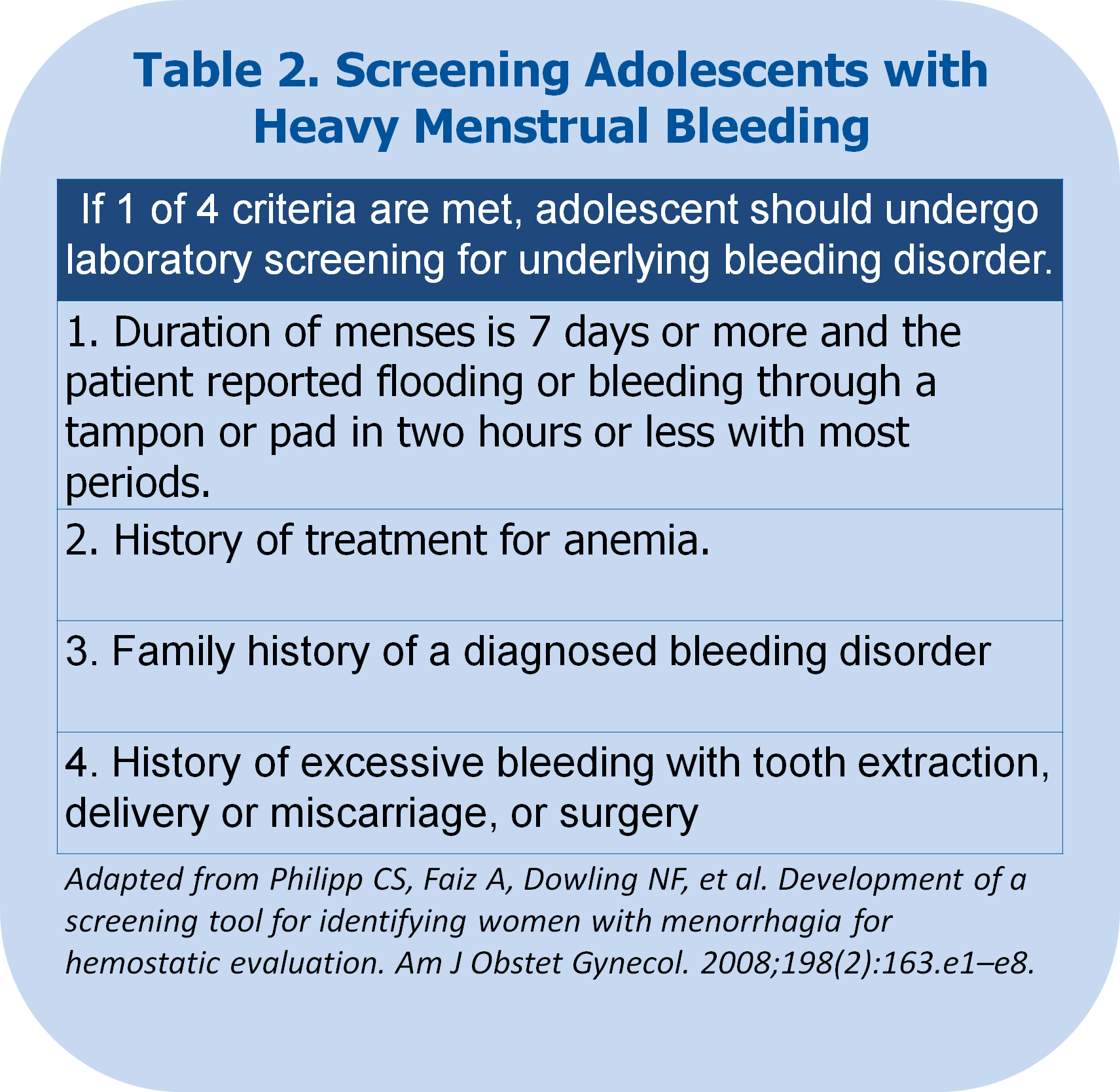
Discussion: Adolescents with heavy menstrual bleeding should have a thorough history to assess risk of bleeding disorder. If patients screen positive for having excessive menstrual bleeding (defined as lasting greater than or equal to seven days and bleeding through a tampon or pad in 2 hours or less), a history of treatment for anemia, a family history of a diagnosed bleeding disorder, or a history of excessive bleeding with procedures or surgery, then the coagulation studies should be performed (Table 2). An elevated INR and PTT that does not correct with mixing studies, is indicative of an inhibitor being present, and should raise concern for a lupus anticoagulant. In patients with heavy menstrual bleeding, oral contraceptive pills are typically the first line treatment. However, patients with lupus anticoagulant are at increased risk of thrombosis, which can be increased further by combined oral contraceptives with estrogen. In this case, the patient was prescribed progestin-only contraceptives to treat her menstrual bleeding to minimize risk of thrombosis.
Conclusions: Adolescents that present with heavy menstrual bleeding and anemia should have a thorough history of screen for risk of a bleeding disorder and if positive undergo coagulation testing. Coagulation testing that does not correct with mixing studies are concerning for an inhibitor being present, such as lupus anticoagulant. For patients with a lupus anticoagulant, treatment with oral contraceptives should be limited to non-estrogen containing formulations to avoid increasing their risk for thrombosis.